- EMS was called — and bystander CPR was promptly started.
- VFib (Ventricular Fibrillation) was documented on arrival by the paramedic team. DC countershock was delivered — with ROSC (Return Of Spontaneous Circulation) and return of the patient to full consciousness.
- The ECG in Figure-1 was obtained following ROSC.
- How would you interpret the ECG in Figure-1?
- Should the cath lab be activated?
-USE.png) |
| Figure-1: The initial ECG in today's case — obtained following ROSC from witnessed cardiac arrest. (To improve visualization — I've digitized the original ECG using PMcardio). |
- The post-ROSC ECG shown in Figure-1 shows sinus tachycardia at 115/minute with a narrow QRS complex rhythm.
- My "eye" was immediately drawn to leads V1,V2 (within the RED rectangle in Figure-2). The marked ST elevation in these leads, with downsloping ST segment into terminal T wave inversion — is diagnostic of a Brugada-1 ECG pattern (See Figure-3 below).
- ST segment straightening, with a somewhat limited amount of ST elevation is seen in neighboring lead V3 (hard to define the J-point in this lead for judging the amount of ST elevation).
- The remainder of this ECG is nonspecific, and surprisingly unremarkable. Small, narrow (and probably insignificant) q waves are seen in the inferior leads. ST segment coving is seen in lead aVL — and minimal J-point depression with an upsloping ST segment is seen in leads V5,V6.
- Sinus tachycardia.
- Brugada-1 ECG pattern in the anterior leads. (I suspect the ST segment straightening with some ST elevation that is seen in neighboring lead V3 reflects a continuation of the Brugada-1 pattern). This is not the ECG of acute infarction!
- Given that this patient is now fully alert — and that there is no history of chest pain — there is no indication for immediate activation of the cath lab.The management plan for this patient should include full investigation for potential precipitating factors of his cardiac arrest (including genetic testing and family history assessment).
- Bottom Line: Given the occurrence cardiac arrest in association with the Brugada-1 pattern on ECG — an ICD (Implantable Cardioverter-Defibrillator) will almost certainly be recomended.
- It turns out that today's patient is of southeast Asian descent. As noted in the ADDENDUM below (See Figure-5) — this geographic area of the world has by far, the highest prevalence of Brugada Syndrome.
- Work-Up of this patient was negative (including normal CT angiography and normal cardiac MRI).
- An ICD was implanted — and the patient was discharged in excellent condition.
-labeled.png) |
| Figure-2: The ST-T wave appearance in leads V1,V2 is diagnostic of a Brugada-1 ECG pattern. |
 |
| Figure-3: Review of ECG Patterns in Brugada Syndrome (adapted from Brugada et al — in JACC 72(9):1046-1059, 2018) — (A) Brugada-1 ECG pattern, showing coved ST-segment elevation ≥2 mm in ≥1 right precordial lead, followed by a negative T-wave. (B) Brugada-2 ECG pattern (the “Saddleback” pattern) — showing concave-up ST-segment elevation ≥0.5 mm (generally ≥2 mm) in ≥1 right precordial lead, followed by a positive T-wave. (C) Additional criteria for diagnosis of a Brugada-2 ECG pattern (TOP: the ß-angle; BOTTOM: A Brugada-2 pattern is present if 5 mm down from the maximum R’ rise point — the base of the triangle formed is ≥4 mm — as this ensures a ß-angle ≥58°). = = = = = = = = = = = = NOTE: Traditionally there have be 3 ECG Brugada patterns described. Newer criteria sometimes "combine" Type-2 and Type-3 into a single "Saddleback" classification for simplicity (which is the classification I favor — and which I show in this Figure). ST-T wave morphology looks similar for Type-2 and Type-3 patterns — but Type-3 Brugada manifests less ST elevation than Type-2 ( = less than 2 mm of J-point elevation — and less than 1 mm of ST elevation). |
- Is the QTc too short?
- As discussed in the review by Rudic et al (Arrhythm Electrophysiol Rev 3(2):76-79, 2014) — SQTS is an inherited cardiac channelopathy determined by the presence of symptoms (syncope, cardiac arrest), positive family history, and the ECG finding of an abnormally short QTc interval.
- SQTS has only been recognized as a distinct clinical entity since 2000. The disorder is rare — but its importance is as a potential cause of atrial and ventricular arrhythmias, including cardiac arrest. Treatment is by ICD.
- Males with a QTc ≤330 msec. (and females with a QTc ≤340 msec.) — are defined as having SQTS, even if they are asymptomatic.
- Males with a QTc ≤360 msec. (and females with a QTc ≤370 msec.) — are said to have a “short” QTc. Such patients may have SQTS if, in addition to the “short” QTc there is a history of cardiac arrest, unexplained syncope or atrial fibrillation at an early age.
- In Figure-4 — I show the values instantly arrived at by our QTc Calculator once you plug in the heart rate (115/minute in today's case) — and once you add in the longest QT that you measure (which is 280 msec. in lead V5).
- As is typically seen — there is some variation in measurements by each of the 5 well-known and established formulas for QTc calculation.
- Whereas in Figure-4 — None of the 5 formulas for QTc calculation come up with an estimated QTc ≤330 msec — both the Fridericia and Framingham methods come up with values below the <360 msec. cutoff for a QTc that is "short" (ie, 348 and 354 msec., respectively).
- Bottom Line: The QTc in today's case is shorter than usual — but is not short enough to qualify as SQTS (keeping in mind the range of QTc values calculated by the different methods — and, that accuracy by any method for QTc estimation is less precise as the heart rate becomes faster).
- P.S.: For discussion of a case of SQTS — Check out My Comment in the Sept 2, 2019 post in Dr. Smith's ECG Blog.
-USE.png) |
| Figure-4: Estimation of the QTc in today's case. The GREEN arrow shows where to find my QTc Calculator in the TOP Menu of every page in this ECG Blog. The lower RIGHT panel shows the values for ECG #1 (given the heart rate = 115/min. — and the measured QT = 280 msec.). Note the range for estimated QTc values (from 348 msec. to 388 msec.) — depending on which of the 5 most commonly used formulas is used. |
- Among references I've used in synthesizing the concepts noted below are El Sayed et al (StatPearls, 2023) — Adytia and Sutanto (Current Prob in Cardiol 49(6), 2024) — Batchvarov (Eur Cardiol 9(2):82-87, 2014) — Netsere et al (BMC Cardiovasc Dis 25, 638, 2025) — and Nakano and Shimizu (JACC Asia 19:2(4):412-421, 2022).
==================================
Acknowledgment: My appreciation to Mubarak Al-Hatemi (from Doha, Qatar) for making me aware of this case and allowing me to use this tracing.
==================================
ADDENDUM (12/13/2025): Summarizing material on Brugada Syndrome:
 |
| Figure-5: 2-page Summary of the essentials of Brugada Syndrome (from my ECG-2014-ePub). |
 |
| Figure-6: World prevalence map of Brugada Syndrome. The overall worldwide prevalence of Brugada Syndrome is ~0.5/1,000 in the population. This prevalence is highest in Southeast Asia (at least 5 timesmore common than in North America). The country with highest prevalence of Brugada Syndrome is Thailand, with ~15 times higher prevalence thn the worldwide average. Brugada-2 patterns (ie, "Saddleback") are also much more prevalent in Southeast Asia than elsewhere in the world. (Excerpted from Vutthikraivit et al: Acta Cardiol Sin 34:267-277, 2018). |
==================
BELOW is FROM ECG Blog #238
https://ecg-interpretation.blogspot.com/2021/07/ecg-blog-238-53-what-is-phenocopy.html
========================
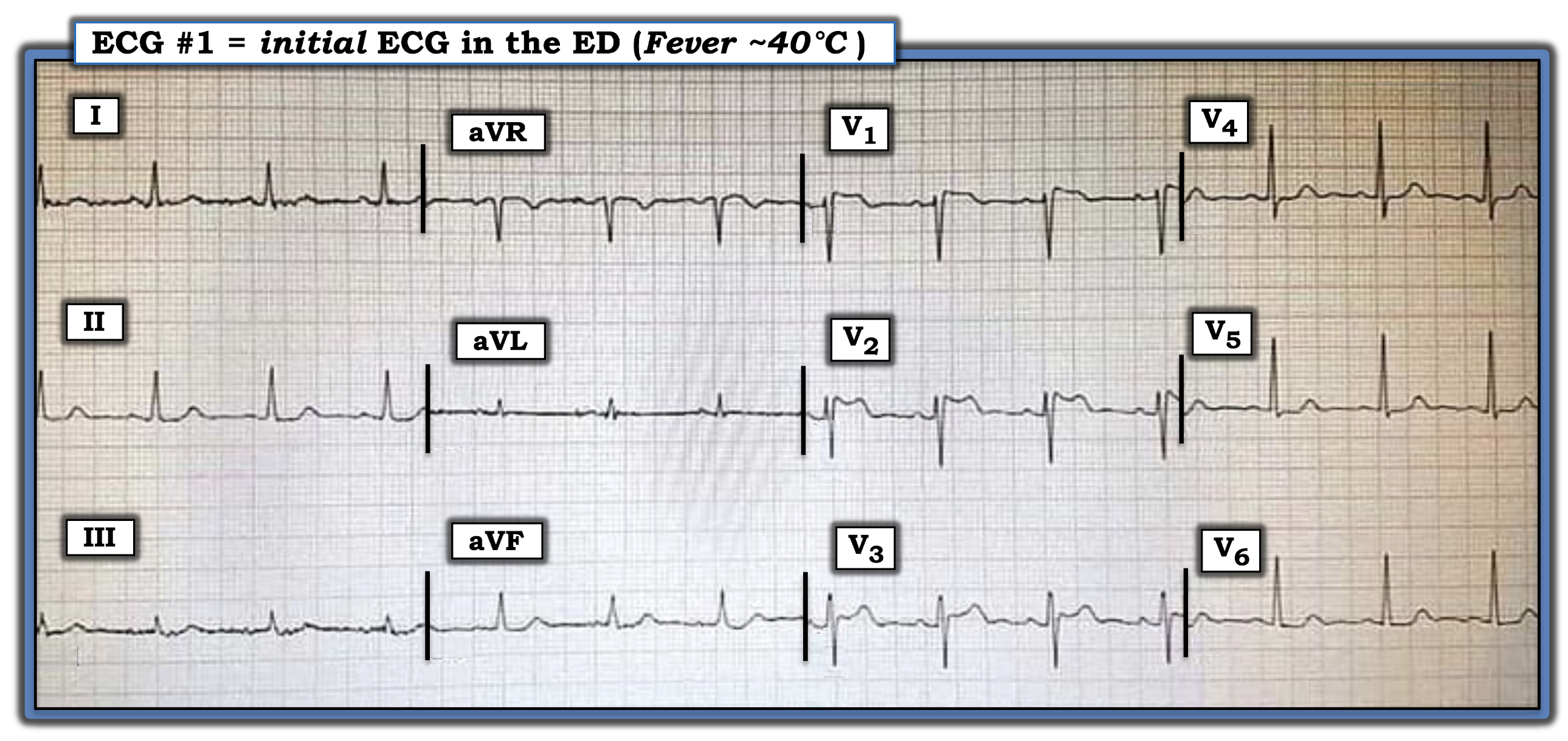
The ECG shown in Figure-1 was obtained from an elderly woman, who presented to the ED (Emergency Department) with an acute febrile illness (40°C).
- How would you interpret her initial ECG?
- Clinically — Could this be an early acute antero-septal STEMI?
 |
| Figure-1: ECG obtained from an elderly woman with an acute febrile illness (See text). |
The Case Continues:
The ECG was repeated (Figure-2) — this time with anterior leads placed 1 interspace higher.
 |
| Figure-2: Repeat ECG of the tracing shown in Figure-1, with anterior leads placed 1 interspace higher (See text). |
QUESTION:
- Do these serial tracings suggest an acute evolving anterior STEMI?
=======================================
NOTE: Some readers may prefer at this point to refer to ECG Media PEARL #53 before reading My Thoughts regarding the ECGs in Figure-2. This 2-part ECG Video (9 minutes and 8 minutes) — reviews the ECG recognition and clinical significance of Brugada-1 and Brugada-2 ECG patterns + it clarifies the concept of Brugada Phenocopy.
- For an excellent state-of-the-art Review article on Brugada Syndrome — CLICK HERE (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018).
- For a Review on the entity of Brugada Phenocopy — CLICK HERE (Anselm D et al: World Cardiol 6(3) 81-86-2014).
- For a study documenting the inability of experts to distinguish between a Brugada-1 ECG pattern from Brugada Syndrome vs Brugada Phenocopy — CLICK HERE (Gottschalk et al: Europace 18, 1095-1100, 2016).
- For brief summary of this material — Please refer to Figures-5, -6 and -7 in the Addendum below.
My THOUGHTS on this Case:
Looking first at the ECG in Figure-1 — The rhythm is sinus — all intervals (PR, QRS, QTc) and the axis are normal — and there is no chamber enlargement.
Regarding Q-R-S-T Changes in Figure-1:
- There are no Q waves.
- R Wave Progression is normal, with transition (where the R wave becomes taller than the S wave is deep) occurring normally between leads V3-to-V4.
- Regarding ST segments and T waves — the most striking abnormality is the ST elevation in leads V1, V2 and V3, with "double-hump" upward concavity in lead V3.
- ST segments are noticeably flattened in several limb leads — as well as in lateral chest leads (that also show slight ST depression).
My Impression of ECG #1: There is no denying the presence of anterior ST elevation with ST segment flattening and slight ST depression in other leads.
- That said — Against these ST-T wave changes in ECG #1 representing an acute cardiac event — is the clinical history of acute febrile illness in this elderly woman, with no mention in the history of associated chest pain.
QUESTION:
What happened in ECG #2 (bottom tracing in Figure-2)?
ANSWER:
The main difference between ECG #1 and ECG #2 is the appearance of the ST-T waves in leads V1, V2 and V3:
- The R' peak in leads V1 and V2 is higher in ECG #2, with sharp downsloping that leads into a more noticeably inverted T wave.
- The "double-hump" upward ST segment concavity that was seen in lead V2 of ECG #1 — is now seen in lead V3 of ECG #2.
My Impression of ECG #2: The ECG picture in Figure-2 stongly suggests we are seeing Brugada ECG patterns.
- The "double-hump" upward ST segment concavity in lead V2 of ECG #1 — is consistent with a Brugada-2 (ie, "Saddleback" ) pattern.
- The higher-rising, steeper downsloping ST-T wave appearance in leads V1 and V2 of ECG #2 — now meets criteria for a Brugada-1 ECG pattern, with a Brugada-2 pattern now seen in lead V3.
- In view of the clinical history — this is unlikely to represent an acute anteroseptal STEMI.
PEARL #1: It turns out that ECG #2 was repeated soon after ECG #1. This illustrates how the simple measure of placing anterior leads 1 or 2 interspaces higher on the chest may serve to bring out a Brugada ECG pattern!
The Case Continues:
The patient was treated for her acute febrile illness. Her ECG was repeated after her fever had resolved (Figure-3).
 |
| Figure-3: Repeat ECG following resolution of this patient's fever — compared to the initial ECG in this case (See text). |
QUESTION:
Does the patient in today's case have Brugada Syndrome?
WHAT is Brugada Syndrome?
First described in 1992 — the Brugada Syndrome is important to recognize because of an associated very high risk of sudden death in otherwise healthy young or middle-aged adults who have structurally normal hearts.
- The prevalence of Brugada Syndrome in the general population is ~1/2,000. The syndrome has become a leading cause of sudden death in young adults (under 40 years of age).
- PEARL #2: Brugada Syndrome is much more common in Southeast Asia compared to the rest of the world. When considering the possibility of this syndrome — demographics of the patient are important! (See Figure-6 in the Addendum below).
- PEARL #3: Although the genetics of Brugada Syndrome are complicated — the gender of the patient is also important. There is a distinct male predominance to this syndrome.
Personal Reflection: I never learned about Brugada Syndrome in medical school (the syndrome had not yet been described). But especially during the past 10 years, in which I've closely followed numerous international ECG internet forums — I've seen countless cases, especially of transient Brugada ECG patterns similar to today's case.
- Once a clinical entity is "discovered" — it begins to get noticed with increasing frequency.
Regarding BRUGADA Syndrome vs Phenocopy:
I reference an excellent state-of-the-art Review article on Brugada Syndrome (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018). I've synthesized key aspects of this article:
- A Brugada Type-1 ECG pattern is diagnosed by the finding of ST elevation of ≥2 mm in one or more of the right precordial leads (ie, V1, V2, V3) — followed by an r’ wave and a coved or straight ST segment — in which the ST segment crosses the isoelectric line and ends in a negative T wave (See Panel A in Figure-4).
- A Brugada-1 pattern may either be observed spontaneously (with leads V1 and/or V2 positioned normally — or — positioned 1 or 2 interspaces higher than usual) — or — a Brugada-1 pattern may be observed as a response to provocative drug testing after IV administration of a sodium-channel blocking agent such as ajmaline, flecainide or procainamide.
- NOTE: In the past, the diagnosis of Brugada Syndrome required not only the presence of a Brugada-1 ECG pattern — but also a history of sudden death, sustained VT, non-vasovagal syncope or a positive family history of sudden death at an early age. This definition was changed following an expert consensus panel in 2013 — so that at the present time, all that is needed to diagnose Brugada Syndrome is a spontaneous or induced Brugada-1 ECG pattern (without need for additional criteria).
- Panel B in Figure-2 illustrates the Brugada Type-2 or "Saddleback" ECG pattern. This pattern may be suggestive — but by itself, it is not diagnostic of Brugada Syndrome (See Figure-4).
|
| Figure-4: Review of ECG Patterns in Brugada Syndrome (adapted from the above cited article by Brugada et al in JACC: Vol 72, Issue 9) — (A) Brugada-1 ECG pattern, showing coved ST-segment elevation ≥2 mm in ≥1 right precordial lead, followed by a negative T-wave. (B) Brugada-2 ECG pattern (the “Saddleback” pattern) — showing concave-up ST-segment elevation ≥0.5 mm (generally ≥2 mm) in ≥1 right precordial lead, followed by a positive T-wave. (C) Additional criteria for diagnosis of a Brugada-2 ECG pattern (TOP: the ß-angle; BOTTOM: A Brugada-2 pattern is present if 5 mm down from the maximum R’ rise point — the base of the triangle formed is ≥4 mm — as this ensures a ß-angle ≥58°). |
PEARL #4: A number of conditions other than Brugada Syndrome may temporarily produce a Brugada-1 ECG pattern. A partial list includes the following:
- Certain drugs (antiarrhythmics; calcium channel blockers; ß-blockers; antianginals; psychotropic medications; alcohol; cocaine; other drugs).
- Acute febrile illness.
- Variations in autonomic tone.
- Hypothermia.
- Electrolyte imbalance (hypokalemia; hyperkalemia).
- Ischemia/infarction.
- Cardioversion/defibrillation.
- Bradycardia.
KEY Point: Development of a Brugada-1 or Brugada-2 ECG pattern as a result of one or more of the above factors — with resolution of this Brugada ECG pattern after correction of the precipitating factor(s) is known as Brugada Phenocopy.
- The importance of being aware of this phenomenon of Brugada Phenocopy — is that correction of the underlying condition (ie, the acute febrile illness in today’s case) may result in resolution of the Brugada-1 ECG pattern — with a much better longterm prognosis compared to patients with true Brugada Syndrome (ie, an ICD may not be needed, as it probably would be if true Brugada Syndrome was present!).
- NOTE: To ensure a diagnosis of Brugada Phenocopy — the patient should have: i) A negative family history of sudden death; ii) Lack of a Brugada-1 ECG pattern in 1st-degree relatives; iii) No history of syncope, serous arrhythmias, seizures or nocturnal agonal respiration; and, iv) A negative sodium channel-blocker challenge test.
==================================
Final Comment on Today's Case:
Assuming the elderly woman in today's case had otherwise been healthy (without a personal history of syncope, serious arrhythmias, seizures or nocturnal agonal respiration) — the fact that the Brugada-1 ECG pattern we initially saw completely resolved so soon after fever resolution, strongly suggests she has Brugada Phenocopy (and not Brugada Syndrome) — and that her longterm prognosis is likely to be good.
- Whether she needs to undergo a negative sodium channel-blocker challenge test at her advanced age (and what impact her family history might have at her age) — are issues for her informed consent and medical providers to decide.
==================================
Acknowledgment: My appreciation to Mubarak Al-Hatemi (from Doha, Qatar) for making me aware of this case and allowing me to use this tracing.
==================================
References & Related ECG Blog Posts to Today’s Case:
- For an excellent state-of-the-art Review article on Brugada Syndrome — CLICK HERE (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018).
- For a Review on the entity of Brugada Phenocopy — CLICK HERE (Anselm D et al: World Cardiol 6(3) 81-86-2014).
- For a study documenting the inability of experts to distinguish between a Brugada-1 ECG pattern from Brugada Syndrome vs Brugada Phenocopy — CLICK HERE (Gottschalk et al: Europace 18, 1095-1100, 2016).
- ECG Blog #50 — For a case of Brugada Syndrome.
- The September 5, 2020 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to see My Comment). This case shows an example of Brugada Phenocopy as a result of Hyperkalemia.
- The May 6, 2019 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to seeMy Comment). This case reviews an example in which it was difficult to distinguish between Brugada Phenocopy vs an ongoing acute STEMI.
- The September 8, 2019 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to see My Comment). This case reviews another example of Brugada Phenocopy as a result of Hyperkalemia.
==================================
ADDENDUM (7/1/2021): Summarizing material on Brugada Syndrome:
|
| Figure-5: 2-page Summary of the essentials of Brugada Syndrome (from my ECG-2014-ePub). |
|
| Figure-6: World prevalence map of Brugada Syndrome. The overall worldwide prevalence of Brugada Syndrome is ~0.5/1,000 in the population. This prevalence is highest in Southeast Asia (at least 5 times more common than in North America). The country with highest prevalence of Brugada Syndrome is Thailand, with ~15 times higher prevalence thn the worldwide average. Brugada-2 patterns (ie, "Saddleback") are also much more prevalent in Southeast Asia than elsewhere in the world. (Excerpted from Vutthikraivit et al: Acta Cardiol Sin 34:267-277, 2018). |
 |
| Figure-7: Summarizing Figure of KEY concepts reviewed in the above ECG Videos (ECG MP-53). |
- EMS was called — and bystander CPR was promptly started.
- VFib (Ventricular Fibrillation) was documented on arrival by the paramedic team. DC countershock was delivered — with ROSC (Return Of Spontaneous Circulation) and return to full consciousness.
- The ECG in Figure-1 was obtained following ROSC.
- How would you interpret the ECG in Figure-1?
- Should the cath lab be activated?
|
| Figure-1: The initial ECG in today's case — obtained following ROSC from witnessed cardiac arrest. (To improve visualization — I've digitized the original ECG using PMcardio). |
- The post-ROSC ECG shown in Figure-1 shows sinus tachycardia at 110/minute with a narrow QRS complex rhythm.
- My "eye" was immediately drawn to leads V1,V2 (within the RED rectangle in Figure-2). The marked ST elevation in these leads, with downsloping ST segment into terminal T wave inversion — is diagnostic of a Brugada-1 ECG pattern (See Figure-3 below).
- ST segment straightening, with a somewhat limited amount of ST elevation is seen in neighboring lead V3 (hard to define the J-point in this lead).
- The remainder of this ECG is nonspecific, and surprisingly unremarkable. Small, narrow (and probably insignificant) q waves are seen in the inferior leads. ST segment coving is seen in lead aVL — and minimal J-point depression with an upsloping ST segment is seen in leads V5,V6.
- Sinus tachycardia.
- Brugada-1 ECG pattern in the anterior leads. (I suspect the ST segment straightening with slight ST elevation seen in neighboring lead V3 reflects a continuation of the Brugada-1 pattern). This is not the ECG of acute infarction!
- Given that this patient is now fully alert — and that there is no history of chest pain — there is no indication for immediate activation of the cath lab.The management plan for this patient should include full investigation for potential precipitating factors of his cardiac arrest (including genetic testing and family history assessment).
- Bottom Line: Given the occurrence cardiac arrest in association with the Brugada-1 pattern on ECG — an ICD (Implantable Cardioverter-Defibrillator) will almost certainly be recomended.
- Today's patient is of southeast Asian descent. As noted in the ADDENDUM below (See Figure-5) — this geographic area of the world has by far, the highest prevalence of Brugada Syndrome.
- Work-Up of this patient was negative (including normal CT angiography and normal cardiac MRI).
- An ICD was implanted — and the patient was discharged in excellent condition.
|
| Figure-2: The ST-T wave appearance in leads V1,V2 is diagnostic of a Brugada-1 ECG pattern. |
|
| Figure-3: Review of ECG Patterns in Brugada Syndrome (adapted from Brugada et al — in JACC 72(9):1046-1059, 2018) — (A) Brugada-1 ECG pattern, showing coved ST-segment elevation ≥2 mm in ≥1 right precordial lead, followed by a negative T-wave. (B) Brugada-2 ECG pattern (the “Saddleback” pattern) — showing concave-up ST-segment elevation ≥0.5 mm (generally ≥2 mm) in ≥1 right precordial lead, followed by a positive T-wave. (C) Additional criteria for diagnosis of a Brugada-2 ECG pattern (TOP: the ß-angle; BOTTOM: A Brugada-2 pattern is present if 5 mm down from the maximum R’ rise point — the base of the triangle formed is ≥4 mm — as this ensures a ß-angle ≥58°). = = = = = = = = = = = = NOTE: Traditionally there have be 3 ECG Brugada Patterns described. Newer criteria sometimes "combine" Type-2 and Type-3 into a single "Saddleback" classification for simplicity (which I favor — and as I show in this Figure). Both Type-2 and Type-3 look similar — but a Type-3 Brugada Pattern manifests less ST elevation (less than 2 mm of J-point elevation — and less than 1 mm of ST elevation). |
- Is the QTc too short?
- As discussed in the review by Rudic et al (Arrhythm Electrophysiol Rev 3(2):76-79, 2014) — SQTS is an inherited cardiac channelopathy determined by the presence of symptoms (syncope, cardiac arrest), positive family history, and the ECG finding of an abnormally short QTc interval.
- SQTS has only been recognized as a distinct clinical entity since 2000. The disorder is rare — but its importance is as a potential cause of atrial and ventricular arrhythmias, including cardiac arrest. Treatment is by ICD.
- To faciliate XXXX
- Males with a QTc ≤330 msec. (and females with a QTc ≤340 msec.) — are defined as having SQTS, even if they are asymptomatic.
- Males with a QTc ≤360 msec. (and females with a QTc ≤370 msec.) — are said to have a “short” QTc. Such patients may have SQTS if, in addition to the “short” QTc there is a history of cardiac arrest, unexplained syncope or atrial fibrillation at an early age.
-USE.png) |
| Figure-4: Estimation of the QTc in today's case. |
==================================
Acknowledgment: My appreciation to Mubarak Al-Hatemi (from Doha, Qatar) for making me aware of this case and allowing me to use this tracing.
==================================
MUBARAK AL-HATEMI <mubarakhatmi88@gmail.com>
— The computer says "Acute MI"—
Good Afternoon Prof. Ken. 9/25/2025 —
I send you this nice case of Brugada syndrome. This ECG belongs to a 35 years old male from southeast Asia. No past medical history witnessed cardiac arrest in the hotel , initiated CPR by security personnel for nearly 5 minutes , when EMS arrived he was in ventricular fibrillation with successful one DC shock and ROSC achieved. Fully recovered.
Plan: ICD insertion.
— Me to check QTc to see if this is SHORT QTc Syndrome? —
NOTE: Mubarak is from Doha, Qatar —
MY REPLY:
Hi. GREAT case that I most probably will use for an ECG Blog — THANK YOU!
I will acknowledge you and let you know when I publish this (may be a little while …).
QUESTION — Was cardiac cath done on this patient? If so — WHEN with respect to his cardiac arrest? (ie, Was it emergent or done after a couple of days).
Again — Excellent teaching case — and very fortunate for this 35yo that he had his arrest where others witnessed it and were able to promptly shock him! — : ) Ken
MY THOUGHTS — Note the ST elevation in V3 and ST coving in aVL — so this patient should have cardiac cath, since acute MI is one of the causes of a Brugada-1 Phenocopy!
REFERENCES:
Batchvarov — Eur Cardiol 9(2):82-87, 2014
https://pmc.ncbi.nlm.nih.gov/articles/PMC6159405/
Netsere et al — BMC Cardiovasc Dis 25, 638, 2025
https://bmccardiovascdisord.biomedcentral.com/articles/10.1186/s12872-025-05102-y
Nakano and Shimizu — JACC Asia 19:2(4):412-421, 2022
https://pmc.ncbi.nlm.nih.gov/articles/PMC9627855/
SSmith — September 2, 2019 post —
https://drsmithsecgblog.com/what-is-differential-of-this-very/
==================================
Acknowledgment: My appreciation to Mubarak Al-Hatemi (from Qatar) for making me aware of this case and allowing me to use this tracing.
==================================
ADDENDUM (12/13/2025): Summarizing material on Brugada Syndrome:
|
| Figure-5: 2-page Summary of the essentials of Brugada Syndrome (from my ECG-2014-ePub). |
|
| Figure-6: World prevalence map of Brugada Syndrome. The overall worldwide prevalence of Brugada Syndrome is ~0.5/1,000 in the population. This prevalence is highest in Southeast Asia (at least 5 timesmore common than in North America). The country with highest prevalence of Brugada Syndrome is Thailand, with ~15 times higher prevalence thn the worldwide average. Brugada-2 patterns (ie, "Saddleback") are also much more prevalent in Southeast Asia than elsewhere in the world. (Excerpted from Vutthikraivit et al: Acta Cardiol Sin 34:267-277, 2018). |
References & Related ECG Blog Posts to Today’s Case:
- For an excellent state-of-the-art Review article on Brugada Syndrome — CLICK HERE (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018).
- For a Review on the entity of Brugada Phenocopy — CLICK HERE (Anselm D et al: World Cardiol 6(3) 81-86-2014).
- For a study documenting the inability of experts to distinguish between a Brugada-1 ECG pattern from Brugada Syndrome vs Brugada Phenocopy — CLICK HERE (Gottschalk et al: Europace 18, 1095-1100, 2016).
- ECG Blog #50 — For a case of Brugada Syndrome.
- The September 5, 2020 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to see My Comment). This case shows an example of Brugada Phenocopy as a result of Hyperkalemia.
- The May 6, 2019 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to seeMy Comment). This case reviews an example in which it was difficult to distinguish between Brugada Phenocopy vs an ongoing acute STEMI.
- The September 8, 2019 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to see My Comment). This case reviews another example of Brugada Phenocopy as a result of Hyperkalemia.
==================================
ADDENDUM (7/1/2021): Summarizing material on Brugada Syndrome:
|
| Figure-5: 2-page Summary of the essentials of Brugada Syndrome (from my ECG-2014-ePub). |
|
| Figure-6: World prevalence map of Brugada Syndrome. The overall worldwide prevalence of Brugada Syndrome is ~0.5/1,000 in the population. This prevalence is highest in Southeast Asia (at least 5 timesmore common than in North America). The country with highest prevalence of Brugada Syndrome is Thailand, with ~15 times higher prevalence thn the worldwide average. Brugada-2 patterns (ie, "Saddleback") are also much more prevalent in Southeast Asia than elsewhere in the world. (Excerpted from Vutthikraivit et al: Acta Cardiol Sin 34:267-277, 2018). |
==================
BELOW is FROM ECG Blog #238
https://ecg-interpretation.blogspot.com/2021/07/ecg-blog-238-53-what-is-phenocopy.html
========================
The ECG shown in Figure-1 was obtained from an elderly woman, who presented to the ED (Emergency Department) with an acute febrile illness (40°C).
- How would you interpret her initial ECG?
- Clinically — Could this be an early acute antero-septal STEMI?
|
| Figure-1: ECG obtained from an elderly woman with an acute febrile illness (See text). |
The Case Continues:
The ECG was repeated (Figure-2) — this time with anterior leads placed 1 interspace higher.
|
| Figure-2: Repeat ECG of the tracing shown in Figure-1, with anterior leads placed 1 interspace higher (See text). |
QUESTION:
- Do these serial tracings suggest an acute evolving anterior STEMI?
=======================================
NOTE: Some readers may prefer at this point to refer to ECG Media PEARL #53 before reading My Thoughts regarding the ECGs in Figure-2. This 2-part ECG Video (9 minutes and 8 minutes) — reviews the ECG recognition and clinical significance of Brugada-1 and Brugada-2 ECG patterns + it clarifies the concept of Brugada Phenocopy.
- For an excellent state-of-the-art Review article on Brugada Syndrome — CLICK HERE (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018).
- For a Review on the entity of Brugada Phenocopy — CLICK HERE (Anselm D et al: World Cardiol 6(3) 81-86-2014).
- For a study documenting the inability of experts to distinguish between a Brugada-1 ECG pattern from Brugada Syndrome vs Brugada Phenocopy — CLICK HERE (Gottschalk et al: Europace 18, 1095-1100, 2016).
- For brief summary of this material — Please refer to Figures-5, -6 and -7 in the Addendum below.
My THOUGHTS on this Case:
Looking first at the ECG in Figure-1 — The rhythm is sinus — all intervals (PR, QRS, QTc) and the axis are normal — and there is no chamber enlargement.
Regarding Q-R-S-T Changes in Figure-1:
- There are no Q waves.
- R Wave Progression is normal, with transition (where the R wave becomes taller than the S wave is deep) occurring normally between leads V3-to-V4.
- Regarding ST segments and T waves — the most striking abnormality is the ST elevation in leads V1, V2 and V3, with "double-hump" upward concavity in lead V3.
- ST segments are noticeably flattened in several limb leads — as well as in lateral chest leads (that also show slight ST depression).
My Impression of ECG #1: There is no denying the presence of anterior ST elevation with ST segment flattening and slight ST depression in other leads.
- That said — Against these ST-T wave changes in ECG #1 representing an acute cardiac event — is the clinical history of acute febrile illness in this elderly woman, with no mention in the history of associated chest pain.
QUESTION:
What happened in ECG #2 (bottom tracing in Figure-2)?
ANSWER:
The main difference between ECG #1 and ECG #2 is the appearance of the ST-T waves in leads V1, V2 and V3:
- The R' peak in leads V1 and V2 is higher in ECG #2, with sharp downsloping that leads into a more noticeably inverted T wave.
- The "double-hump" upward ST segment concavity that was seen in lead V2 of ECG #1 — is now seen in lead V3 of ECG #2.
My Impression of ECG #2: The ECG picture in Figure-2 stongly suggests we are seeing Brugada ECG patterns.
- The "double-hump" upward ST segment concavity in lead V2 of ECG #1 — is consistent with a Brugada-2 (ie, "Saddleback" ) pattern.
- The higher-rising, steeper downsloping ST-T wave appearance in leads V1 and V2 of ECG #2 — now meets criteria for a Brugada-1 ECG pattern, with a Brugada-2 pattern now seen in lead V3.
- In view of the clinical history — this is unlikely to represent an acute anteroseptal STEMI.
PEARL #1: It turns out that ECG #2 was repeated soon after ECG #1. This illustrates how the simple measure of placing anterior leads 1 or 2 interspaces higher on the chest may serve to bring out a Brugada ECG pattern!
The Case Continues:
The patient was treated for her acute febrile illness. Her ECG was repeated after her fever had resolved (Figure-3).
|
| Figure-3: Repeat ECG following resolution of this patient's fever — compared to the initial ECG in this case (See text). |
QUESTION:
Does the patient in today's case have Brugada Syndrome?
WHAT is Brugada Syndrome?
First described in 1992 — the Brugada Syndrome is important to recognize because of an associated very high risk of sudden death in otherwise healthy young or middle-aged adults who have structurally normal hearts.
- The prevalence of Brugada Syndrome in the general population is ~1/2,000. The syndrome has become a leading cause of sudden death in young adults (under 40 years of age).
- PEARL #2: Brugada Syndrome is much more common in Southeast Asia compared to the rest of the world. When considering the possibility of this syndrome — demographics of the patient are important! (See Figure-6 in the Addendum below).
- PEARL #3: Although the genetics of Brugada Syndrome are complicated — the gender of the patient is also important. There is a distinct male predominance to this syndrome.
Personal Reflection: I never learned about Brugada Syndrome in medical school (the syndrome had not yet been described). But especially during the past 10 years, in which I've closely followed numerous international ECG internet forums — I've seen countless cases, especially of transient Brugada ECG patterns similar to today's case.
- Once a clinical entity is "discovered" — it begins to get noticed with increasing frequency.
Regarding BRUGADA Syndrome vs Phenocopy:
I reference an excellent state-of-the-art Review article on Brugada Syndrome (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018). I've synthesized key aspects of this article:
- A Brugada Type-1 ECG pattern is diagnosed by the finding of ST elevation of ≥2 mm in one or more of the right precordial leads (ie, V1, V2, V3) — followed by an r’ wave and a coved or straight ST segment — in which the ST segment crosses the isoelectric line and ends in a negative T wave (See Panel A in Figure-4).
- A Brugada-1 pattern may either be observed spontaneously (with leads V1 and/or V2 positioned normally — or — positioned 1 or 2 interspaces higher than usual) — or — a Brugada-1 pattern may be observed as a response to provocative drug testing after IV administration of a sodium-channel blocking agent such as ajmaline, flecainide or procainamide.
- NOTE: In the past, the diagnosis of Brugada Syndrome required not only the presence of a Brugada-1 ECG pattern — but also a history of sudden death, sustained VT, non-vasovagal syncope or a positive family history of sudden death at an early age. This definition was changed following an expert consensus panel in 2013 — so that at the present time, all that is needed to diagnose Brugada Syndrome is a spontaneous or induced Brugada-1 ECG pattern (without need for additional criteria).
- Panel B in Figure-2 illustrates the Brugada Type-2 or "Saddleback" ECG pattern. This pattern may be suggestive — but by itself, it is not diagnostic of Brugada Syndrome (See Figure-4).
|
| Figure-4: Review of ECG Patterns in Brugada Syndrome (adapted from the above cited article by Brugada et al in JACC: Vol 72, Issue 9) — (A) Brugada-1 ECG pattern, showing coved ST-segment elevation ≥2 mm in ≥1 right precordial lead, followed by a negative T-wave. (B) Brugada-2 ECG pattern (the “Saddleback” pattern) — showing concave-up ST-segment elevation ≥0.5 mm (generally ≥2 mm) in ≥1 right precordial lead, followed by a positive T-wave. (C) Additional criteria for diagnosis of a Brugada-2 ECG pattern (TOP: the ß-angle; BOTTOM: A Brugada-2 pattern is present if 5 mm down from the maximum R’ rise point — the base of the triangle formed is ≥4 mm — as this ensures a ß-angle ≥58°). |
PEARL #4: A number of conditions other than Brugada Syndrome may temporarily produce a Brugada-1 ECG pattern. A partial list includes the following:
- Certain drugs (antiarrhythmics; calcium channel blockers; ß-blockers; antianginals; psychotropic medications; alcohol; cocaine; other drugs).
- Acute febrile illness.
- Variations in autonomic tone.
- Hypothermia.
- Electrolyte imbalance (hypokalemia; hyperkalemia).
- Ischemia/infarction.
- Cardioversion/defibrillation.
- Bradycardia.
KEY Point: Development of a Brugada-1 or Brugada-2 ECG pattern as a result of one or more of the above factors — with resolution of this Brugada ECG pattern after correction of the precipitating factor(s) is known as Brugada Phenocopy.
- The importance of being aware of this phenomenon of Brugada Phenocopy — is that correction of the underlying condition (ie, the acute febrile illness in today’s case) may result in resolution of the Brugada-1 ECG pattern — with a much better longterm prognosis compared to patients with true Brugada Syndrome (ie, an ICD may not be needed, as it probably would be if true Brugada Syndrome was present!).
- NOTE: To ensure a diagnosis of Brugada Phenocopy — the patient should have: i) A negative family history of sudden death; ii) Lack of a Brugada-1 ECG pattern in 1st-degree relatives; iii) No history of syncope, serous arrhythmias, seizures or nocturnal agonal respiration; and, iv) A negative sodium channel-blocker challenge test.
==================================
Final Comment on Today's Case:
Assuming the elderly woman in today's case had otherwise been healthy (without a personal history of syncope, serious arrhythmias, seizures or nocturnal agonal respiration) — the fact that the Brugada-1 ECG pattern we initially saw completely resolved so soon after fever resolution, strongly suggests she has Brugada Phenocopy (and not Brugada Syndrome) — and that her longterm prognosis is likely to be good.
- Whether she needs to undergo a negative sodium channel-blocker challenge test at her advanced age (and what impact her family history might have at her age) — are issues for her informed consent and medical providers to decide.
==================================
Acknowledgment: My appreciation to Mubarak Al-Hatemi (from Doha, Qatar) for making me aware of this case and allowing me to use this tracing.
==================================
References & Related ECG Blog Posts to Today’s Case:
- For an excellent state-of-the-art Review article on Brugada Syndrome — CLICK HERE (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018).
- For a Review on the entity of Brugada Phenocopy — CLICK HERE (Anselm D et al: World Cardiol 6(3) 81-86-2014).
- For a study documenting the inability of experts to distinguish between a Brugada-1 ECG pattern from Brugada Syndrome vs Brugada Phenocopy — CLICK HERE (Gottschalk et al: Europace 18, 1095-1100, 2016).
- ECG Blog #50 — For a case of Brugada Syndrome.
- The September 5, 2020 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to see My Comment). This case shows an example of Brugada Phenocopy as a result of Hyperkalemia.
- The May 6, 2019 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to seeMy Comment). This case reviews an example in which it was difficult to distinguish between Brugada Phenocopy vs an ongoing acute STEMI.
- The September 8, 2019 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to see My Comment). This case reviews another example of Brugada Phenocopy as a result of Hyperkalemia.
==================================
ADDENDUM (7/1/2021): Summarizing material on Brugada Syndrome:
|
| Figure-5: 2-page Summary of the essentials of Brugada Syndrome (from my ECG-2014-ePub). |
|
| Figure-6: World prevalence map of Brugada Syndrome. The overall worldwide prevalence of Brugada Syndrome is ~0.5/1,000 in the population. This prevalence is highest in Southeast Asia (at least 5 times more common than in North America). The country with highest prevalence of Brugada Syndrome is Thailand, with ~15 times higher prevalence thn the worldwide average. Brugada-2 patterns (ie, "Saddleback") are also much more prevalent in Southeast Asia than elsewhere in the world. (Excerpted from Vutthikraivit et al: Acta Cardiol Sin 34:267-277, 2018). |
|
| Figure-7: Summarizing Figure of KEY concepts reviewed in the above ECG Videos (ECG MP-53). |
References & Related ECG Blog Posts to Today’s Case:
- For an excellent state-of-the-art Review article on Brugada Syndrome — CLICK HERE (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018).
- For a Review on the entity of Brugada Phenocopy — CLICK HERE (Anselm D et al: World Cardiol 6(3) 81-86-2014).
- For a study documenting the inability of experts to distinguish between a Brugada-1 ECG pattern from Brugada Syndrome vs Brugada Phenocopy — CLICK HERE (Gottschalk et al: Europace 18, 1095-1100, 2016).
- ECG Blog #50 — For a case of Brugada Syndrome.
- The September 5, 2020 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to see My Comment). This case shows an example of Brugada Phenocopy as a result of Hyperkalemia.
- The May 6, 2019 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to seeMy Comment). This case reviews an example in which it was difficult to distinguish between Brugada Phenocopy vs an ongoing acute STEMI.
- The September 8, 2019 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to see My Comment). This case reviews another example of Brugada Phenocopy as a result of Hyperkalemia.
==================================
ADDENDUM (7/1/2021): Summarizing material on Brugada Syndrome:
|
| Figure-5: 2-page Summary of the essentials of Brugada Syndrome (from my ECG-2014-ePub). |
|
| Figure-6: World prevalence map of Brugada Syndrome. The overall worldwide prevalence of Brugada Syndrome is ~0.5/1,000 in the population. This prevalence is highest in Southeast Asia (at least 5 timesmore common than in North America). The country with highest prevalence of Brugada Syndrome is Thailand, with ~15 times higher prevalence thn the worldwide average. Brugada-2 patterns (ie, "Saddleback") are also much more prevalent in Southeast Asia than elsewhere in the world. (Excerpted from Vutthikraivit et al: Acta Cardiol Sin 34:267-277, 2018). |
==================
BELOW is FROM ECG Blog #238
https://ecg-interpretation.blogspot.com/2021/07/ecg-blog-238-53-what-is-phenocopy.html
========================
The ECG shown in Figure-1 was obtained from an elderly woman, who presented to the ED (Emergency Department) with an acute febrile illness (40°C).
- How would you interpret her initial ECG?
- Clinically — Could this be an early acute antero-septal STEMI?
|
| Figure-1: ECG obtained from an elderly woman with an acute febrile illness (See text). |
The Case Continues:
The ECG was repeated (Figure-2) — this time with anterior leads placed 1 interspace higher.
|
| Figure-2: Repeat ECG of the tracing shown in Figure-1, with anterior leads placed 1 interspace higher (See text). |
QUESTION:
- Do these serial tracings suggest an acute evolving anterior STEMI?
=======================================
NOTE: Some readers may prefer at this point to refer to ECG Media PEARL #53 before reading My Thoughts regarding the ECGs in Figure-2. This 2-part ECG Video (9 minutes and 8 minutes) — reviews the ECG recognition and clinical significance of Brugada-1 and Brugada-2 ECG patterns + it clarifies the concept of Brugada Phenocopy.
- For an excellent state-of-the-art Review article on Brugada Syndrome — CLICK HERE (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018).
- For a Review on the entity of Brugada Phenocopy — CLICK HERE (Anselm D et al: World Cardiol 6(3) 81-86-2014).
- For a study documenting the inability of experts to distinguish between a Brugada-1 ECG pattern from Brugada Syndrome vs Brugada Phenocopy — CLICK HERE (Gottschalk et al: Europace 18, 1095-1100, 2016).
- For brief summary of this material — Please refer to Figures-5, -6 and -7 in the Addendum below.
My THOUGHTS on this Case:
Looking first at the ECG in Figure-1 — The rhythm is sinus — all intervals (PR, QRS, QTc) and the axis are normal — and there is no chamber enlargement.
Regarding Q-R-S-T Changes in Figure-1:
- There are no Q waves.
- R Wave Progression is normal, with transition (where the R wave becomes taller than the S wave is deep) occurring normally between leads V3-to-V4.
- Regarding ST segments and T waves — the most striking abnormality is the ST elevation in leads V1, V2 and V3, with "double-hump" upward concavity in lead V3.
- ST segments are noticeably flattened in several limb leads — as well as in lateral chest leads (that also show slight ST depression).
My Impression of ECG #1: There is no denying the presence of anterior ST elevation with ST segment flattening and slight ST depression in other leads.
- That said — Against these ST-T wave changes in ECG #1 representing an acute cardiac event — is the clinical history of acute febrile illness in this elderly woman, with no mention in the history of associated chest pain.
QUESTION:
What happened in ECG #2 (bottom tracing in Figure-2)?
ANSWER:
The main difference between ECG #1 and ECG #2 is the appearance of the ST-T waves in leads V1, V2 and V3:
- The R' peak in leads V1 and V2 is higher in ECG #2, with sharp downsloping that leads into a more noticeably inverted T wave.
- The "double-hump" upward ST segment concavity that was seen in lead V2 of ECG #1 — is now seen in lead V3 of ECG #2.
My Impression of ECG #2: The ECG picture in Figure-2 stongly suggests we are seeing Brugada ECG patterns.
- The "double-hump" upward ST segment concavity in lead V2 of ECG #1 — is consistent with a Brugada-2 (ie, "Saddleback" ) pattern.
- The higher-rising, steeper downsloping ST-T wave appearance in leads V1 and V2 of ECG #2 — now meets criteria for a Brugada-1 ECG pattern, with a Brugada-2 pattern now seen in lead V3.
- In view of the clinical history — this is unlikely to represent an acute anteroseptal STEMI.
PEARL #1: It turns out that ECG #2 was repeated soon after ECG #1. This illustrates how the simple measure of placing anterior leads 1 or 2 interspaces higher on the chest may serve to bring out a Brugada ECG pattern!
The Case Continues:
The patient was treated for her acute febrile illness. Her ECG was repeated after her fever had resolved (Figure-3).
|
| Figure-3: Repeat ECG following resolution of this patient's fever — compared to the initial ECG in this case (See text). |
QUESTION:
Does the patient in today's case have Brugada Syndrome?
WHAT is Brugada Syndrome?
First described in 1992 — the Brugada Syndrome is important to recognize because of an associated very high risk of sudden death in otherwise healthy young or middle-aged adults who have structurally normal hearts.
- The prevalence of Brugada Syndrome in the general population is ~1/2,000. The syndrome has become a leading cause of sudden death in young adults (under 40 years of age).
- PEARL #2: Brugada Syndrome is much more common in Southeast Asia compared to the rest of the world. When considering the possibility of this syndrome — demographics of the patient are important! (See Figure-6 in the Addendum below).
- PEARL #3: Although the genetics of Brugada Syndrome are complicated — the gender of the patient is also important. There is a distinct male predominance to this syndrome.
Personal Reflection: I never learned about Brugada Syndrome in medical school (the syndrome had not yet been described). But especially during the past 10 years, in which I've closely followed numerous international ECG internet forums — I've seen countless cases, especially of transient Brugada ECG patterns similar to today's case.
- Once a clinical entity is "discovered" — it begins to get noticed with increasing frequency.
Regarding BRUGADA Syndrome vs Phenocopy:
I reference an excellent state-of-the-art Review article on Brugada Syndrome (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018). I've synthesized key aspects of this article:
- A Brugada Type-1 ECG pattern is diagnosed by the finding of ST elevation of ≥2 mm in one or more of the right precordial leads (ie, V1, V2, V3) — followed by an r’ wave and a coved or straight ST segment — in which the ST segment crosses the isoelectric line and ends in a negative T wave (See Panel A in Figure-4).
- A Brugada-1 pattern may either be observed spontaneously (with leads V1 and/or V2 positioned normally — or — positioned 1 or 2 interspaces higher than usual) — or — a Brugada-1 pattern may be observed as a response to provocative drug testing after IV administration of a sodium-channel blocking agent such as ajmaline, flecainide or procainamide.
- NOTE: In the past, the diagnosis of Brugada Syndrome required not only the presence of a Brugada-1 ECG pattern — but also a history of sudden death, sustained VT, non-vasovagal syncope or a positive family history of sudden death at an early age. This definition was changed following an expert consensus panel in 2013 — so that at the present time, all that is needed to diagnose Brugada Syndrome is a spontaneous or induced Brugada-1 ECG pattern (without need for additional criteria).
- Panel B in Figure-2 illustrates the Brugada Type-2 or "Saddleback" ECG pattern. This pattern may be suggestive — but by itself, it is not diagnostic of Brugada Syndrome (See Figure-4).
|
| Figure-4: Review of ECG Patterns in Brugada Syndrome (adapted from the above cited article by Brugada et al in JACC: Vol 72, Issue 9) — (A) Brugada-1 ECG pattern, showing coved ST-segment elevation ≥2 mm in ≥1 right precordial lead, followed by a negative T-wave. (B) Brugada-2 ECG pattern (the “Saddleback” pattern) — showing concave-up ST-segment elevation ≥0.5 mm (generally ≥2 mm) in ≥1 right precordial lead, followed by a positive T-wave. (C) Additional criteria for diagnosis of a Brugada-2 ECG pattern (TOP: the ß-angle; BOTTOM: A Brugada-2 pattern is present if 5 mm down from the maximum R’ rise point — the base of the triangle formed is ≥4 mm — as this ensures a ß-angle ≥58°). |
PEARL #4: A number of conditions other than Brugada Syndrome may temporarily produce a Brugada-1 ECG pattern. A partial list includes the following:
- Certain drugs (antiarrhythmics; calcium channel blockers; ß-blockers; antianginals; psychotropic medications; alcohol; cocaine; other drugs).
- Acute febrile illness.
- Variations in autonomic tone.
- Hypothermia.
- Electrolyte imbalance (hypokalemia; hyperkalemia).
- Ischemia/infarction.
- Cardioversion/defibrillation.
- Bradycardia.
KEY Point: Development of a Brugada-1 or Brugada-2 ECG pattern as a result of one or more of the above factors — with resolution of this Brugada ECG pattern after correction of the precipitating factor(s) is known as Brugada Phenocopy.
- The importance of being aware of this phenomenon of Brugada Phenocopy — is that correction of the underlying condition (ie, the acute febrile illness in today’s case) may result in resolution of the Brugada-1 ECG pattern — with a much better longterm prognosis compared to patients with true Brugada Syndrome (ie, an ICD may not be needed, as it probably would be if true Brugada Syndrome was present!).
- NOTE: To ensure a diagnosis of Brugada Phenocopy — the patient should have: i) A negative family history of sudden death; ii) Lack of a Brugada-1 ECG pattern in 1st-degree relatives; iii) No history of syncope, serous arrhythmias, seizures or nocturnal agonal respiration; and, iv) A negative sodium channel-blocker challenge test.
==================================
Final Comment on Today's Case:
Assuming the elderly woman in today's case had otherwise been healthy (without a personal history of syncope, serious arrhythmias, seizures or nocturnal agonal respiration) — the fact that the Brugada-1 ECG pattern we initially saw completely resolved so soon after fever resolution, strongly suggests she has Brugada Phenocopy (and not Brugada Syndrome) — and that her longterm prognosis is likely to be good.
- Whether she needs to undergo a negative sodium channel-blocker challenge test at her advanced age (and what impact her family history might have at her age) — are issues for her informed consent and medical providers to decide.
==================================
Acknowledgment: My appreciation to Mubarak Al-Hatemi (from Doha, Qatar) for making me aware of this case and allowing me to use this tracing.
==================================
References & Related ECG Blog Posts to Today’s Case:
- For an excellent state-of-the-art Review article on Brugada Syndrome — CLICK HERE (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018).
- For a Review on the entity of Brugada Phenocopy — CLICK HERE (Anselm D et al: World Cardiol 6(3) 81-86-2014).
- For a study documenting the inability of experts to distinguish between a Brugada-1 ECG pattern from Brugada Syndrome vs Brugada Phenocopy — CLICK HERE (Gottschalk et al: Europace 18, 1095-1100, 2016).
- ECG Blog #50 — For a case of Brugada Syndrome.
- The September 5, 2020 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to see My Comment). This case shows an example of Brugada Phenocopy as a result of Hyperkalemia.
- The May 6, 2019 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to seeMy Comment). This case reviews an example in which it was difficult to distinguish between Brugada Phenocopy vs an ongoing acute STEMI.
- The September 8, 2019 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to see My Comment). This case reviews another example of Brugada Phenocopy as a result of Hyperkalemia.
==================================
ADDENDUM (7/1/2021): Summarizing material on Brugada Syndrome:
|
| Figure-5: 2-page Summary of the essentials of Brugada Syndrome (from my ECG-2014-ePub). |
|
| Figure-6: World prevalence map of Brugada Syndrome. The overall worldwide prevalence of Brugada Syndrome is ~0.5/1,000 in the population. This prevalence is highest in Southeast Asia (at least 5 times more common than in North America). The country with highest prevalence of Brugada Syndrome is Thailand, with ~15 times higher prevalence thn the worldwide average. Brugada-2 patterns (ie, "Saddleback") are also much more prevalent in Southeast Asia than elsewhere in the world. (Excerpted from Vutthikraivit et al: Acta Cardiol Sin 34:267-277, 2018). |
|
| Figure-7: Summarizing Figure of KEY concepts reviewed in the above ECG Videos (ECG MP-53). |
Brugada syndrome is a rare but potentially life-threatening inherited disease that predisposes patients to fatal cardiac arrhythmias. The syndrome is characterized by the ECG findings of a right bundle branch block and ST-segment elevations in the right precordial leads (V1-V3). This activity outlines the evaluation and management of Brugada syndrome and explains the roles of the interprofessional team in caring for patients with patients with Brugada syndrome.
Objectives:
- Describe the etiology and epidemiology of Brugada syndrome.
- Summarize the pathophysiology of Brugada syndrome.
- Outline the typical presentation and evaluation of a patient with Brugada syndrome.
- Explain the importance of improving care coordination among the interprofessional team to improve outcomes for patients affected by Brugada syndrome.
Introduction
Brugada syndrome is a genetic disease that predisposes patients to fatal cardiac arrhythmias. It is named after Josep and Pedro Brugada who first described it in 1992. The syndrome is characterized by the ECG findings of a right bundle branch block and ST-segment elevations in the right precordial leads (V1-V3). [1]
Etiology
The first genetic association with Brugada syndrome discovered was a loss-of-function mutation in the cardiac voltage-gated sodium channel gene SCN5A. It is thought to be found in 15-30% of Brugada Syndrome cases. [2] Mutations in calcium and potassium channels, associated channel proteins, and desmosomal proteins have also been linked with the disease. Brugada syndrome is inherited in an autosomal dominant pattern; however, affected individuals may demonstrate variable expressivity and reduced penetrance. Additionally, many environmental and genetic factors may influence the phenotype, including temperature, medications, electrolyte abnormalities, and cocaine.[3]
Epidemiology
The prevalence of Brugada Syndrome is approximately 3 to 5 per 10,000 people. Brugada syndrome is approximately 8 to 10 times more common in males than females. This gender difference, however, is not found in pediatric patients. This has been hypothesized to be due to higher testosterone levels after puberty and different proportions of ionic currents based on sex. Brugada syndrome is also more prevalent in those who are of Southeast Asian descent. The mean affected age is 41 years old. Brugada syndrome accounts for 4% of all sudden cardiac deaths. [3]
Pathophysiology
The exact mechanism for Brugada Syndrome is not clear. There are two main physiologic hypotheses that have been suggested: the repolarization disorder and the depolarization disorder models. According to the repolarization disorder model, the decrease in sodium current secondary to the loss-of-function sodium channel mutation causes the right ventricular epicardium's action potential to have a deeper notch when compared to the action potential of the endocardium. This difference in current can lead to the typical EKG finding of Brugada syndrome and subsequent fatal arrhythmias. The depolarization disorder model, on the other hand, suggests that the EKG findings of Brugada syndrome are secondary to a delay in depolarization due to slow conduction in the right ventricular outflow tract.
Histopathology
When Brugada syndrome was first described, it was thought to be only in structurally normal hearts. However, newer research revealed right ventricular outflow tract abnormalities, such as an increase in adipose tissue and fibrosis. These structural abnormalities support the depolarization disorder model as a possible cause of slower conduction in the right ventricular outflow tract. Nonetheless, whether these structural abnormalities account for the arrhythmias caused in Brugada syndrome or that they are the result of the disease and aging process is still a matter of debate. [4]
History and Physical
Symptoms of Brugada syndrome range from the absence of any symptoms to sudden cardiac death. Sudden cardiac death typically occurs during sleep, possibly secondary to increased vagal tone. Approximately 80% of Brugada syndrome patients who develop ventricular tachycardia or ventricular fibrillation experience syncope. Palpitations and dizziness have also been described as possible symptoms. History of a febrile illness may be present as fever may precipitate symptoms and arrhythmias. 10 to 30% of Brugada syndrome patients will have an atrial arrhythmia, and supraventricular tachycardia is also more common in Brugada syndrome patients than the general population. However, 72% of those with Brugada syndrome will not show any symptoms, and 28% will not have a family history of sudden cardiac death.
Evaluation
A 12-lead electrocardiogram is significant to both diagnose and decide management options of Brugada syndrome. Three different ECG patterns have been described in Brugada syndrome patients: coved ST elevations greater than 2 mm accompanied with an inverted T wave (type I), saddleback-shaped ST elevation greater than 2 mm (type II), and saddle-back shaped ST elevations less than 2 mm (type III). Additionally, patients with a normal ECG and high-risk factors may require a drug challenge test to reveal the typical ECG findings of ST elevations in the precordial leads V1 to V3. These high-risk factors that may require provocative drug testings include having a family history of Brugada syndrome, family history of sudden cardiac death, and symptoms consistent with Brugada syndrome in the setting of questionable ECG abnormalities. [3]
Class IA antiarrhythmics (such as procainamide and ajmaline) and IC antiarrhythmics (such as flecainide and propafenone), which act as sodium channel blockers, are the drugs used in the challenge test. Brugada ECG findings may also be revealed after cocaine use or tricyclic antidepressant toxicity. Electrolyte abnormalities, such as hyperkalemia and hypercalcemia have been known to reveal ST elevations in the right precordial leads.[5]
If a drug challenge test is normal in a pediatric patient, it may require repetition after the child reaches puberty, given the hormonal effects on Brugada syndrome phenotype. Another diagnostic test described to expose the ST elevations of Brugada syndrome is the full stomach test, where ECGs are obtained before and after a large meal, which causes an increase in vagal tone. Other tests that may be useful for some patients include genetic testing for SCN5A mutations and invasive electrophysiology. [3]
Treatment / Management
An implantable cardioverter-defibrillator (ICD) is the mainstay of treatment of Brugada syndrome patients. Current recommendations are to perform ICD placement in those who survived cardiac arrest, patients with Brugada ECG abnormalities and syncope, and those who can have Brugada ECG findings on drug challenge tests. Pharmacological treatment with quinidine is also an option. There are conflicting results about using quinidine instead of ICD placement; however, quinidine is useful in Brugada syndrome patients with an ICD who experience multiple shocks and in those who have contraindications for ICD placement. Finally, radio frequency ablation of the anterior part of the right ventricular outflow tract is a new, emerging therapy with a promising prognosis for Brugada syndrome patients. Treatment of asymptomatic individuals with Brugada syndrome ECG findings is more complicated. Personalized risk-stratification is essential in providing the right management for these asymptomatic patients depending on their risk factors using a multi-disciplinary approach and with close and frequent follow-up. [6]
Differential Diagnosis
Many of the conditions that may be mistaken for Brugada syndrome also cause syncope as a common symptom. Standard of care for evaluation of syncope is to obtain a 12-lead ECG to evaluate for many of such diseases that may resemble Brugada syndrome. These diseases include QT prolongation, Wolff-Parkinson-White syndrome, pulmonary embolism, sick sinus syndrome, early repolarization syndrome, electrolyte abnormalities, and atrial fibrillation. [3]
Enhancing Healthcare Team Outcomes
Brugada syndrome is not very common, but because it is associated with sudden death, it is important for healthcare workers to be aware of the ECG presentation. The disorder is best managed by an interprofessional team that includes a cardiologist, electrophysiologist and a genetic counselor. The key to diagnosis is a comprehensive medical history of syncopal attacks, chest discomfort or dizziness. Once the diagnosis is made, patients need to be educated about the potential for cardiac arrest. While an ICD is routinely implanted in these patients, it also predisposes them to device-related complications and inappropriate shocks. The actual incidence of death from Brugada syndrome is not known but may account for 3-20% of all sudden deaths in patients with structurally normal hearts. Sudden deaths tend to occur early after the fourth decade of life. The patient, family, and coworkers must be educated about the basics of CPR. Once the diagnosis of Brugada syndrome is made, genetic counseling should be offered to the family.[7][8](Level V)
==========================
BELOW is AI Summary — Should an athlete with Type-2 Brugada pattern be allowed to do sports?
can often play sports, especially if asymptomatic, but requires thorough, individualized risk assessment (stress tests, genetics) to rule out higher-risk Type-1 BrP, with guidelines generally allowing participation if low-risk (asymptomatic, no family history, negative electrophysiology study), but requiring ICD/restriction for syncope/cardiac arrest history, always emphasizing hydration, avoiding fever/certain drugs, and having emergency plans.
- Asymptomatic Status: Being symptom-free (no fainting, palpitations during exertion) is crucial for clearance.
- Risk Stratification is Key: A cardiologist must conduct tests like exercise stress testing and potentially electrophysiology (EP) studies to differentiate low-risk Type-2 from potentially dangerous Type-1 patterns.
- Type 2 vs. Type 1: Type-2 patterns (which often disappear with higher heart rates) are generally considered lower risk than Type-1, but a spontaneous Type-1 appearing during stress testing can indicate high risk.
- Family History: A history of sudden cardiac death (SCD) in the family raises the risk significantly.
- American Heart Association/ESC Guidelines: Allow competitive sports for asymptomatic individuals with Type 2/3 patterns, provided no other risk factors exist.
- Asymptomatic athlete.
- Type 2 or 3 pattern on ECG.
- No personal history of fainting (syncope) or cardiac arrest.
- No family history of SCD.
- Negative or inconclusive EP study (if performed).
- History of syncope or cardiac arrest.
- Spontaneous Type-1 pattern.
- Presence of other risk factors or a positive EP study.
- Avoid Triggers: Stay hydrated, avoid fever, and stay cool during exercise.
- Medication Avoidance: Know and avoid drugs that can trigger BrS (refer to resources like BrugadaDrugs.org).
- Emergency Plan: Have an Automated External Defibrillator (AED) accessible and an emergency action plan in place with team officials
===========================
BELOW — CITE this GREAT AJC article !!!!
KEY POINT: The presence of a Type 2/3 BrP is not diagnostic alone for BrS and it has been described as highly prevalent as 12% in the athletic population, especially in endurance athletes, partially linked to the extreme exercise-induced right ventricular (RV) enlargement.19 Common features for BrP and early repolarization are the male prevalence, vagal influence and normalization with quinidine. Moreover, improper recording of the ECG with high pass filtering and high placement of the precordial lead can cause a rSr' pattern, but not a baseline Type 1 BrP, in athletes and in the general population.20Misplaced leads can generate the need of additional exams and unnecessary sport restriction, especially in tall endurance athletes.
Genetic testing for Brugada syndrome (BrS) is currently recommended in subjects with (1) spontaneous or (2) pharmacologically induced type I pattern, in association with clinical features (such as polymorphic ventricular tachycardia, ventricular fibrillation, arrhythmic syncope) or family history, to support the diagnosis.1 It should be requested by a cardiologist or a physician with specific knowledge in BrS, particularly after excluding phenocopies and known confounding factors.21
=================
|
| Figure-1: The initial ECG in today's case — obtained from a patient XXXX (To improve visualization — I've digitized the original ECG using PMcardio). |
|
| Figure-2: XXX |
|
| Figure-3: Review of ECG Patterns in Brugada Syndrome (adapted from the above cited article by Brugada et al in JACC: Vol 72, Issue 9) — (A) Brugada-1 ECG pattern, showing coved ST-segment elevation ≥2 mm in ≥1 right precordial lead, followed by a negative T-wave. (B) Brugada-2 ECG pattern (the “Saddleback” pattern) — showing concave-up ST-segment elevation ≥0.5 mm (generally ≥2 mm) in ≥1 right precordial lead, followed by a positive T-wave. (C) Additional criteria for diagnosis of a Brugada-2 ECG pattern (TOP: the ß-angle; BOTTOM: A Brugada-2 pattern is present if 5 mm down from the maximum R’ rise point — the base of the triangle formed is ≥4 mm — as this ensures a ß-angle ≥58°). = = = = = = = = = = = = NOTE: Traditionally there have be 3 ECG Brugada Patterns described. Newer criteria sometimes "combine" Type-2 and Type-3 into a single "Saddleback" classification for simplicity (which I favor — and as I show in this Figure). Both Type-2 and Type-3 look similar — but a Type-3 Brugada Pattern manifests less ST elevation (less than 2 mm of J-point elevation — and less than 1 mm of ST elevation). |
|
| Figure-4: Estimation of the QTc in today's case. |
- As emphasized in this article — SQTS is an inherited cardiac channelopathy determined by the presence of symptoms (syncope, cardiac arrest), positive family history, and the ECG finding of an abnormally short QTc interval.
- SQTS is a relatively new diagnosis that has only been recognized as a distinct clinical entity since 2000. The disorder is rare — but its importance is as a potential cause of atrial and ventricular arrhythmias, including cardiac arrest. Treatment is by ICD (implantable cardioverter defibrillator).
- Males with a QTc ≤330 msec. (and females with a QTc ≤340 msec.) — are defined as having SQTS, even if they are asymptomatic.
- Males with a QTc ≤360 msec. (and females with a QTc ≤370 msec.) — are said to have a “short” QTc. Such patients may have SQTS if, in addition to the “short” QTc there is a history of cardiac arrest, unexplained syncope or atrial fibrillation at an early age.
MUBARAK AL-HATEMI <mubarakhatmi88@gmail.com>
— The computer says "Acute MI"—
Good Afternoon Prof. Ken. 9/25/2025 —
I send you this nice case of Brugada syndrome. This ECG belongs to a 35 years old male from southeast Asia. No past medical history witnessed cardiac arrest in the hotel , initiated CPR by security personnel for nearly 5 minutes , when EMS arrived he was in ventricular fibrillation with successful one DC shock and ROSC achieved. Fully recovered.
Plan: ICD insertion.
— Me to check QTc to see if this is SHORT QTc Syndrome? —
NOTE: Mubarak is from Doha, Qatar —
MY REPLY:
Hi. GREAT case that I most probably will use for an ECG Blog — THANK YOU!
I will acknowledge you and let you know when I publish this (may be a little while …).
QUESTION — Was cardiac cath done on this patient? If so — WHEN with respect to his cardiac arrest? (ie, Was it emergent or done after a couple of days).
Again — Excellent teaching case — and very fortunate for this 35yo that he had his arrest where others witnessed it and were able to promptly shock him! — : ) Ken
MY THOUGHTS — Note the ST elevation in V3 and ST coving in aVL — so this patient should have cardiac cath, since acute MI is one of the causes of a Brugada-1 Phenocopy!
REFERENCES:
Batchvarov — Eur Cardiol 9(2):82-87, 2014
https://pmc.ncbi.nlm.nih.gov/articles/PMC6159405/
Netsere et al — BMC Cardiovasc Dis 25, 638, 2025
https://bmccardiovascdisord.biomedcentral.com/articles/10.1186/s12872-025-05102-y
Nakano and Shimizu — JACC Asia 19:2(4):412-421, 2022
https://pmc.ncbi.nlm.nih.gov/articles/PMC9627855/
SSmith — September 2, 2019 post —
https://drsmithsecgblog.com/what-is-differential-of-this-very/
==================================
Acknowledgment: My appreciation to Mubarak Al-Hatemi (from Qatar) for making me aware of this case and allowing me to use this tracing.
==================================
References & Related ECG Blog Posts to Today’s Case:
- For an excellent state-of-the-art Review article on Brugada Syndrome — CLICK HERE (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018).
- For a Review on the entity of Brugada Phenocopy — CLICK HERE (Anselm D et al: World Cardiol 6(3) 81-86-2014).
- For a study documenting the inability of experts to distinguish between a Brugada-1 ECG pattern from Brugada Syndrome vs Brugada Phenocopy — CLICK HERE (Gottschalk et al: Europace 18, 1095-1100, 2016).
- ECG Blog #50 — For a case of Brugada Syndrome.
- The September 5, 2020 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to see My Comment). This case shows an example of Brugada Phenocopy as a result of Hyperkalemia.
- The May 6, 2019 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to seeMy Comment). This case reviews an example in which it was difficult to distinguish between Brugada Phenocopy vs an ongoing acute STEMI.
- The September 8, 2019 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to see My Comment). This case reviews another example of Brugada Phenocopy as a result of Hyperkalemia.
==================================
ADDENDUM (7/1/2021): Summarizing material on Brugada Syndrome:
|
| Figure-5: 2-page Summary of the essentials of Brugada Syndrome (from my ECG-2014-ePub). |
|
| Figure-6: World prevalence map of Brugada Syndrome. The overall worldwide prevalence of Brugada Syndrome is ~0.5/1,000 in the population. This prevalence is highest in Southeast Asia (at least 5 timesmore common than in North America). The country with highest prevalence of Brugada Syndrome is Thailand, with ~15 times higher prevalence thn the worldwide average. Brugada-2 patterns (ie, "Saddleback") are also much more prevalent in Southeast Asia than elsewhere in the world. (Excerpted from Vutthikraivit et al: Acta Cardiol Sin 34:267-277, 2018). |
|
| Figure-7: Summarizing Figure of KEY concepts reviewed in the above ECG Videos (ECG MP-53). |
==================
BELOW is FROM ECG Blog #238
https://ecg-interpretation.blogspot.com/2021/07/ecg-blog-238-53-what-is-phenocopy.html
========================
The ECG shown in Figure-1 was obtained from an elderly woman, who presented to the ED (Emergency Department) with an acute febrile illness (40°C).
- How would you interpret her initial ECG?
- Clinically — Could this be an early acute antero-septal STEMI?
|
| Figure-1: ECG obtained from an elderly woman with an acute febrile illness (See text). |
The Case Continues:
The ECG was repeated (Figure-2) — this time with anterior leads placed 1 interspace higher.
|
| Figure-2: Repeat ECG of the tracing shown in Figure-1, with anterior leads placed 1 interspace higher (See text). |
QUESTION:
- Do these serial tracings suggest an acute evolving anterior STEMI?
=======================================
NOTE: Some readers may prefer at this point to refer to ECG Media PEARL #53 before reading My Thoughts regarding the ECGs in Figure-2. This 2-part ECG Video (9 minutes and 8 minutes) — reviews the ECG recognition and clinical significance of Brugada-1 and Brugada-2 ECG patterns + it clarifies the concept of Brugada Phenocopy.
- For an excellent state-of-the-art Review article on Brugada Syndrome — CLICK HERE (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018).
- For a Review on the entity of Brugada Phenocopy — CLICK HERE (Anselm D et al: World Cardiol 6(3) 81-86-2014).
- For a study documenting the inability of experts to distinguish between a Brugada-1 ECG pattern from Brugada Syndrome vs Brugada Phenocopy — CLICK HERE (Gottschalk et al: Europace 18, 1095-1100, 2016).
- For brief summary of this material — Please refer to Figures-5, -6 and -7 in the Addendum below.
=======================================

My THOUGHTS on this Case:
Looking first at the ECG in Figure-1 — The rhythm is sinus — all intervals (PR, QRS, QTc) and the axis are normal — and there is no chamber enlargement.
Regarding Q-R-S-T Changes in Figure-1:
- There are no Q waves.
- R Wave Progression is normal, with transition (where the R wave becomes taller than the S wave is deep) occurring normally between leads V3-to-V4.
- Regarding ST segments and T waves — the most striking abnormality is the ST elevation in leads V1, V2 and V3, with "double-hump" upward concavity in lead V3.
- ST segments are noticeably flattened in several limb leads — as well as in lateral chest leads (that also show slight ST depression).
My Impression of ECG #1: There is no denying the presence of anterior ST elevation with ST segment flattening and slight ST depression in other leads.
- That said — Against these ST-T wave changes in ECG #1 representing an acute cardiac event — is the clinical history of acute febrile illness in this elderly woman, with no mention in the history of associated chest pain.
QUESTION:
What happened in ECG #2 (bottom tracing in Figure-2)?
ANSWER:
The main difference between ECG #1 and ECG #2 is the appearance of the ST-T waves in leads V1, V2 and V3:
- The R' peak in leads V1 and V2 is higher in ECG #2, with sharp downsloping that leads into a more noticeably inverted T wave.
- The "double-hump" upward ST segment concavity that was seen in lead V2 of ECG #1 — is now seen in lead V3 of ECG #2.
My Impression of ECG #2: The ECG picture in Figure-2 stongly suggests we are seeing Brugada ECG patterns.
- The "double-hump" upward ST segment concavity in lead V2 of ECG #1 — is consistent with a Brugada-2 (ie, "Saddleback" ) pattern.
- The higher-rising, steeper downsloping ST-T wave appearance in leads V1 and V2 of ECG #2 — now meets criteria for a Brugada-1 ECG pattern, with a Brugada-2 pattern now seen in lead V3.
- In view of the clinical history — this is unlikely to represent an acute anteroseptal STEMI.
PEARL #1: It turns out that ECG #2 was repeated soon after ECG #1. This illustrates how the simple measure of placing anterior leads 1 or 2 interspaces higher on the chest may serve to bring out a Brugada ECG pattern!
The Case Continues:
The patient was treated for her acute febrile illness. Her ECG was repeated after her fever had resolved (Figure-3).
|
| Figure-3: Repeat ECG following resolution of this patient's fever — compared to the initial ECG in this case (See text). |
QUESTION:
Does the patient in today's case have Brugada Syndrome?
WHAT is Brugada Syndrome?
First described in 1992 — the Brugada Syndrome is important to recognize because of an associated very high risk of sudden death in otherwise healthy young or middle-aged adults who have structurally normal hearts.
- The prevalence of Brugada Syndrome in the general population is ~1/2,000. The syndrome has become a leading cause of sudden death in young adults (under 40 years of age).
- PEARL #2: Brugada Syndrome is much more common in Southeast Asia compared to the rest of the world. When considering the possibility of this syndrome — demographics of the patient are important! (See Figure-6 in the Addendum below).
- PEARL #3: Although the genetics of Brugada Syndrome are complicated — the gender of the patient is also important. There is a distinct male predominance to this syndrome.
Personal Reflection: I never learned about Brugada Syndrome in medical school (the syndrome had not yet been described). But especially during the past 10 years, in which I've closely followed numerous international ECG internet forums — I've seen countless cases, especially of transient Brugada ECG patterns similar to today's case.
- Once a clinical entity is "discovered" — it begins to get noticed with increasing frequency.
Regarding BRUGADA Syndrome vs Phenocopy:
I reference an excellent state-of-the-art Review article on Brugada Syndrome (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018). I've synthesized key aspects of this article:
- A Brugada Type-1 ECG pattern is diagnosed by the finding of ST elevation of ≥2 mm in one or more of the right precordial leads (ie, V1, V2, V3) — followed by an r’ wave and a coved or straight ST segment — in which the ST segment crosses the isoelectric line and ends in a negative T wave (See Panel A in Figure-4).
- A Brugada-1 pattern may either be observed spontaneously (with leads V1 and/or V2 positioned normally — or — positioned 1 or 2 interspaces higher than usual) — or — a Brugada-1 pattern may be observed as a response to provocative drug testing after IV administration of a sodium-channel blocking agent such as ajmaline, flecainide or procainamide.
- NOTE: In the past, the diagnosis of Brugada Syndrome required not only the presence of a Brugada-1 ECG pattern — but also a history of sudden death, sustained VT, non-vasovagal syncope or a positive family history of sudden death at an early age. This definition was changed following an expert consensus panel in 2013 — so that at the present time, all that is needed to diagnose Brugada Syndrome is a spontaneous or induced Brugada-1 ECG pattern (without need for additional criteria).
- Panel B in Figure-2 illustrates the Brugada Type-2 or "Saddleback" ECG pattern. This pattern may be suggestive — but by itself, it is not diagnostic of Brugada Syndrome (See Figure-4).
|
| Figure-4: Review of ECG Patterns in Brugada Syndrome (adapted from the above cited article by Brugada et al in JACC: Vol 72, Issue 9) — (A) Brugada-1 ECG pattern, showing coved ST-segment elevation ≥2 mm in ≥1 right precordial lead, followed by a negative T-wave. (B) Brugada-2 ECG pattern (the “Saddleback” pattern) — showing concave-up ST-segment elevation ≥0.5 mm (generally ≥2 mm) in ≥1 right precordial lead, followed by a positive T-wave. (C) Additional criteria for diagnosis of a Brugada-2 ECG pattern (TOP: the ß-angle; BOTTOM: A Brugada-2 pattern is present if 5 mm down from the maximum R’ rise point — the base of the triangle formed is ≥4 mm — as this ensures a ß-angle ≥58°). |
PEARL #4: A number of conditions other than Brugada Syndrome may temporarily produce a Brugada-1 ECG pattern. A partial list includes the following:
- Certain drugs (antiarrhythmics; calcium channel blockers; ß-blockers; antianginals; psychotropic medications; alcohol; cocaine; other drugs).
- Acute febrile illness.
- Variations in autonomic tone.
- Hypothermia.
- Electrolyte imbalance (hypokalemia; hyperkalemia).
- Ischemia/infarction.
- Cardioversion/defibrillation.
- Bradycardia.
KEY Point: Development of a Brugada-1 or Brugada-2 ECG pattern as a result of one or more of the above factors — with resolution of this Brugada ECG pattern after correction of the precipitating factor(s) is known as Brugada Phenocopy.
- The importance of being aware of this phenomenon of Brugada Phenocopy — is that correction of the underlying condition (ie, the acute febrile illness in today’s case) may result in resolution of the Brugada-1 ECG pattern — with a much better longterm prognosis compared to patients with true Brugada Syndrome (ie, an ICD may not be needed, as it probably would be if true Brugada Syndrome was present!).
- NOTE: To ensure a diagnosis of Brugada Phenocopy — the patient should have: i) A negative family history of sudden death; ii) Lack of a Brugada-1 ECG pattern in 1st-degree relatives; iii) No history of syncope, serous arrhythmias, seizures or nocturnal agonal respiration; and, iv) A negative sodium channel-blocker challenge test.
==================================
Final Comment on Today's Case:
Assuming the elderly woman in today's case had otherwise been healthy (without a personal history of syncope, serious arrhythmias, seizures or nocturnal agonal respiration) — the fact that the Brugada-1 ECG pattern we initially saw completely resolved so soon after fever resolution, strongly suggests she has Brugada Phenocopy (and not Brugada Syndrome) — and that her longterm prognosis is likely to be good.
- Whether she needs to undergo a negative sodium channel-blocker challenge test at her advanced age (and what impact her family history might have at her age) — are issues for her informed consent and medical providers to decide.
==================================
Acknowledgment: My appreciation to 유영준 (from Seoul, Korea) for making me aware of this case and allowing me to use this tracing.
==================================
References & Related ECG Blog Posts to Today’s Case:
- For an excellent state-of-the-art Review article on Brugada Syndrome — CLICK HERE (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018).
- For a Review on the entity of Brugada Phenocopy — CLICK HERE (Anselm D et al: World Cardiol 6(3) 81-86-2014).
- For a study documenting the inability of experts to distinguish between a Brugada-1 ECG pattern from Brugada Syndrome vs Brugada Phenocopy — CLICK HERE (Gottschalk et al: Europace 18, 1095-1100, 2016).
- ECG Blog #50 — For a case of Brugada Syndrome.
- The September 5, 2020 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to see My Comment). This case shows an example of Brugada Phenocopy as a result of Hyperkalemia.
- The May 6, 2019 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to seeMy Comment). This case reviews an example in which it was difficult to distinguish between Brugada Phenocopy vs an ongoing acute STEMI.
- The September 8, 2019 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to see My Comment). This case reviews another example of Brugada Phenocopy as a result of Hyperkalemia.
==================================
ADDENDUM (7/1/2021): Summarizing material on Brugada Syndrome:
|
| Figure-5: 2-page Summary of the essentials of Brugada Syndrome (from my ECG-2014-ePub). |
|
| Figure-6: World prevalence map of Brugada Syndrome. The overall worldwide prevalence of Brugada Syndrome is ~0.5/1,000 in the population. This prevalence is highest in Southeast Asia (at least 5 timesmore common than in North America). The country with highest prevalence of Brugada Syndrome is Thailand, with ~15 times higher prevalence thn the worldwide average. Brugada-2 patterns (ie, "Saddleback") are also much more prevalent in Southeast Asia than elsewhere in the world. (Excerpted from Vutthikraivit et al: Acta Cardiol Sin 34:267-277, 2018). |
|
| Figure-7: Summarizing Figure of KEY concepts reviewed in the above ECG Videos (ECG MP-53). |
No comments:
Post a Comment