MY Comment, by KEN GRAUER, MD (1/16/2027):
- Today's patient unfortunately developed PEA (Pulseless Electrical Activity) arrest shortly after arrival of the medic team. Although we lack details of events that followed — Dr. Smith makes the key point that had this arrest witnessed by the medic team been the result of an acute cardiac event (therefore, presumably VT or VFib) — prompt defibrillation by on-the-scene medics would most probably have resuscitated her.
- PEA is uncommon as an initial rhythm witnessed by EMS on the scene when the cause is an acute ischemic event. Therefore (as emphasized by Dr. Smith) — when OHCA (Out-of-Hospital Cardiac Arrest) is witnessed by EMS and the patient immediately becomes comatose — Think of a cause other than acute MI or VT/VFib as the reason for the arrest!
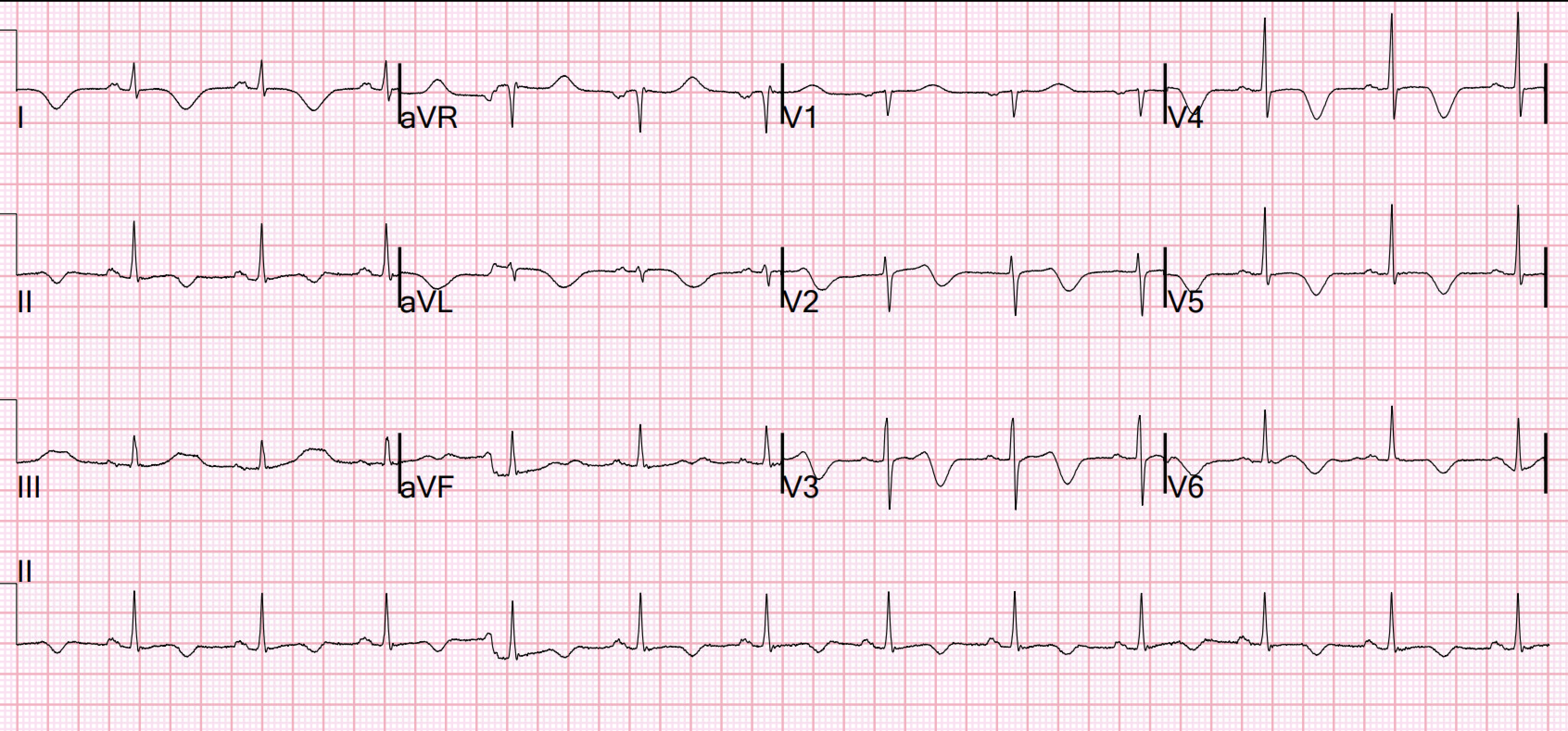
- There is sinus tachycardia at ~115/minute.
- The QTc looks prolonged (well over half the R-R interval) — although accurate QTc assessment becomes challenging at this rapid a rate.
- The most striking finding is the diffuse, profound ST elevation (that attains >8 mm in lead V4! ).
- There is ST elevation in 9/12 leads — with ST depression only seen in lead aVR>V1 (ie, virtually the opposite of what is seen with diffuse subendocardial ischemia — in which there is diffuse ST depression except for ST elevation in aVR>V1).
- As per Dr. Smith — Cardiac cath was negative — and today's unfortunate patient succumbed from her devastating SAH (SubArachnoid Hemorrhage).
- In my experience — CNS catastrophes (not only SAH or other CNS bleeds — but brain tumor — trauma — seizures — coma from other cause) may cause some of the most bizarre-appearing ECGs. Mistaking such cases as an acute cardiac event is not uncommon because of these ECG changes. Awareness of the potential as an "MI mimic" in these cases is essential for avoiding unnecessary cardiac catheterizations that may delay potential lifesaving treatment.
.png) |
| Figure-1: Comparison between the initial ECG in today's case (TOP) — with the initial ECG from the December 20, 2021 post, in which the patient also suffered a lethal subarachnoid hemorrhage. |
- Less diffuse and less marked ST elevation in association with reciprocal ST depression in the inferior leads — illustrates how closely some CNS bleeds may resemble acute OMI.
- Once again — the History proved KEY in pointing to the diagnosis (ie, this patient collapsed, but never lost a pulse — and despite prompt electrical cardioversion she remained deeply comatose).
- ECG abnormalities are extremely common with SAH (seemingly much more so than with other types of CNS bleeds). Percentages in the papers I reviewed vary, depending on criteria that were chosen for "ECG abnormalities". That said — the "theme" is that ECG abnormalities are an expected finding, especially with SAH.
- QTc prolongation seems to be the most common abnormality found — but T wave abnormalities (sometimes "Giant" T waves) — ST segment deviations (both elevation and depression, albeit ST depression seems to be more common with SAH according to the literature I reviewed) — and on occasion, Osborn waves and/or U waves.
- A full range of rhythm disorders may be seen — including sinus tachycardia and sinus bradycardia ( = opposite ends of the spectrum — perhaps depending on whether there is still increased sympathetic tone — or whether the patient is now decompensating with increased intracerebral pressure) — as well as the gamut of SVT rhythms and ventricular rhythms (including VT).
- The mechanism for ECG abnormalities with SAH is uncertain — but most investigators point to a central increase in sympathetic tone (ie, catecholamine surge — that either results in myocardium "stunning" or autonomic deregulation).
- Papers I reviewed include — (Poudel et al — Cureus 15(6): e40045, 2023) — (Chatterjee — Neth Heart J 19:31-34, 2011) — (Yogendranathan et al — BMC Cardiovasc Dis 17(91)- 2017) — (Ibrahim and Macdonald — Stroke 43(8): 2102-2107, 2012) — (Levis — Permanente J 21:16-049, 2017).
-USE.png) |
| Figure-1: The initial ECG in today's case. (To improve visualization — I've digitized the original ECG using PMcardio). |
SAH case Buerk
syncope. 911. medics arrive and patient goes into PEA arrest. Resuscitated without defibrillation.

I was wondering your thoughts on this EKG. It was a patient who came in after a syncopal event and then witnessed PEA arrest by medics. She went to cath lab but had a clean cath and it ended up being a devastating SAH after pcomm aneurysm rupture. I was wondering if there was any clues on the EKG that it would not be an OMI and if you would have sent her to the cath lab with that story.
It is the clinical presentation that gives the most information.
The big clue on the EKG is that there is huge ST elevation everywhere. This only occurs with coronary occlusion that would affect inferior, high lateral, low lateral walls, or if it is takotsubo (which is identical to the findings that you see with intracranial events). There is no way to make this distinction on the EKG.
The big CLINICAL clue to the diagnosis are these 2 things:
1) the patient had a PEA arrest in front of the medics. I would bet that she was in a coma when they resuscitated her. Ischemic arrests are almost always V Fib arrest (except when prolonged, because eventually VF becomes PEA, but in this case they witnessed that the first event was PEA)
2) patients who have arrest witnessed by medics from Coronary occlusion are resuscitated quickly and do not usually have deep coma.

Was she in deep coma when she arrived? (These patients almost always are — never seen one that is awake)


No comments:
Post a Comment