MY Comment, by KEN GRAUER, MD (1/5/2025):
- Grauer: Because my "ECG brain" has been wired for interpretation of ECGs at the 25 mm/second speed (that is standard in the U.S. and in most of the world) — My routine is to selectively reduce the width of such tracings by 50% to compensate for the 50 mm/second speed routinely used with the Cabrera format. This has been done in Figure-1.
- Outlined in BLUE just above lead V1 — are several ECG grid boxes to facilitate recognizing that the R-R interval in ECG #1 is approximately 3 large boxes in duration — corresponding to a rate of ~100/minute for the rhythm in Figure-1.
- Given globalization of our world — we favor familiarization with different recording formats (For detailed review of the Cabrera Format — Check out Dr. Grauer's Comment at the bottom of the page in the October 26, 2020 post in Dr. Smith's ECG Blog).
- Other than sinus rhythm — What else do you see in ECG #1?
-USE.png) |
| Figure-1: The initial ECG in today's case. |
- The rate of ~100/minute would be fast for an 80-something year old adult — unless something acute is going on (or unless there is really 2:1 AV conduction).
- And, IF the upright deflection in lead V1 was a sinus P wave — then the PR interval would be longer-than-expected for a tachycardic rhythm. Of course, there could be sinus rhythm with 1st-degree AV block — but by the "Bix" Rule — whenever the PR interval looks longer-than-it-should-be for a supraventricular rhythm — there may be another P wave hidden within the QRS complex! (For more on the "Bix" Rule — See My Comment July 16, 2024 post).
- There is no distinct, upright P wave in lead II. Instead, other than in lead V1 — what we see are indistinct broad, low amplitude deflections in many leads. KEY Point: Unless there is lead reversal or dextrocardia — a clear, upright P wave should always be upright in lead II if the rhythm is sinus.
- Sinus P waves are usually not all positive in lead V1 (unless there is RAA).
- The presence of a pseudo-r' deflection in lead V1 (as we see in Figure-2) — is a common "hiding place" for either extra or retrograde P waves.
- Grauer: My “Go To” Leads when looking for less obvious atrial activity in a supraventricular rhythm — are leads II and V1 (as the best leads to look at first) — but also leads III, aVF and aVR, each of which may be surprisingly helpful for finding retrograde P waves or flutter waves.
- Despite this QRS widening, the rhythm in Figure-2 "looks" to be supraventricular (with a nonspecific conduction defect accounting for the QRS widening) — especially given the finding of 2:1 atrial activity, in which the PR interval stays constant before each QRS (which strongly suggests that every-other-P-wave is conducting).
- That said — ST-T waves do not suggest acute ischemia in this tracing.
- The rhythm in Figure-2 appears to be supraventricular with 2:1 AV conduction.
- The ventricular rate is ~100/minute.
- Since there are 2 P waves within each R-R interval — the atrial rate must be twice the ventricular rate, or ~200/minute.
- Therefore, the differential diagnosis in Figure-2 is between: i) ATach (Atrial Tachycardia) vs ii) AFlutter (Atrial Flutter). Although a subtle "sawtooth" pattern does appear to be present in the inferior leads — a ventricular response of ~200/minute would be slow for untreated AFlutter ...
-USE.png) |
| Figure-2: Colored arrows highlight flutter waves, with 2:1 AV conduction. |
- On questioning — the patient reports intermittent palpitations in recent months.
- He was admitted to the hospital with a suspected diagnosis of SSS (Sick Sinus Syndrome). This was based on spells of tachycardia (accounting for palpitations) — with tachycardia espisodes being frequently interrupted by bradycardic episodes (as the probable cause for this patient's syncope at rest). (For review of assessment for SSS — See My Comments in the June 5, 2018 post and the January 22, 2020 post).
- Nossen: I initially saw the ECG in Figure-1, knowing only that the patient was an elderly man on Flecainide, who presented to the ED for syncope. I was told that an episode of a wide tachycardia was captured on telemetry. However, having seen the 2:1 atrial activity in lead V1 (RED arrows in Figure-2) — I was not at all convinced that the episode was VT.
-USE.png) |
| Figure-3: Rhythm captured on telemetry. (Recording speed = 25 mm/second.) |
- Although there is possible indication of intermittent atrial activity (vs artifact) — no clear P waves are seen. A diagnosis of VT (Ventricular Tachycardia) was assumed.
- Nossen: But the patient is on Flecainide ...
-USE.png) |
| Figure-4: Spontaneous conversion of the WCT in Figure-3. (Recording speed = 25 mm/second.) |
- Do you agree that the WCT rhythm is VT?
- What other possible explanations might there be?
- Will you recommend ICD placement for this patient?
- Nossen: I was suspicious that the underlying rhythm was AFlutter throughout the above clinical scenario. Use of Flecainide could account for the slower-than-expected flutter rate of ~200/minute that we saw in Figure-2. And perhaps once the flutter rate dropped below 200/minute — 1:1 AV conduction of AFlutter became possible, with the marked increase in QRS widening that we see in Figure-4 being attributed to Flecainide toxicity. Therefore — no VT — but instead, 1:1 AFlutter with Flecainide-induced QRS widening!
-USE.png) |
| Figure-5: An earlier telemetry recording |
Impression of Figure-5:
- As was the case for today's initial ECG — the QRS is not nearly as wide as it became in Figure-3.
- For parts of the rhythm in Figure-4 — the R-R interval looks regular. But in other parts of this tracing — the R-R interval varies.
- As was the case in Figure-2 — distinct atrial activity is best seen in lead V1 (RED arrows in Figure-6). Once again, atrial activity is much more difficult to make out in other leads. That said — regular flutter waves at 180/minute are seen in Figure-6!
-P_waves-USE.png) |
| Figure-6: I've labeled atrial activity in ECG #4. |
- Grauer: It is common for AFlutter to manifest periods of group beating due to dual-level Wenckebach conduction out of the AV node. Despite consecutively non-conducted flutter waves — this is not a conduction "block" — but rather an expected reduced conduction by an AV node presented with too many rapid flutter impulses to be able to conduct them all.
- The intricate relationships prevalent with dual-level AV conduction are easiest to appreciate by means of a laddergram — which I show in Figure-7. Many combinations of Wenckebach conduction out of 2 or more levels within the AV node are possible (ie, the relationships illustrated in my Figure-7 laddergram do not represent the only possibility).
- The "good news" — is that Wenckebach conduction out of the AV node is usually not a fixed (ie, pathologic) conduction defect. Instead — the chances are excellent that normal AV conduction will resume once sinus rhythm is restored!
- For more on dual-level block with AFlutter — See My Comments in the June 3, 2024 post — the November 24, 2020 post — and the October 25, 2021 post.
- Note that even after resolution of the WCT rhythm in Figure-4 — the QRS remains wide with similar (albeit not identical) QRS morphology in each of the 7 leads of this rhythm strip. I suspect much of the difference in QRS morphology between the WCT rhythm and the rhythm after spontaneous conversion — is the result of the slower rate.
- Note especially that after spontaneous conversion of the WCT rhythm in Figure-4 — that there is a slight but-definitely-present irregularity in the slower post-conversion rhythm. I suspect the entire Figure-4 tracing reflects AFlutter — initially with 1:1 AV conduction — and after rate slowing, with variable AV conduction by a mechanism similar to that which I show in my Figure-7 laddergram. (Unfortunately — there is no lead V1 recording in Figure-4, which is really the only lead that shows distinct flutter wave activity in this patient).
-USE.png) |
| Figure-7: Proposed laddergram for ECG #4 (See text). |
=====================================
- Among potential manifestations of Flecainide Toxicity are: i) QRS widening, which may be marked — often with bizarre QRS morphology that does not resemble any known form of conduction block; ii) Slowing of conduction in atrial and ventricular tissue, as well as in the His-Purkinje system; iii) VT — as a proarrhythmic effect; and, iv) Facilitating conversion of AFib to AFlutter — as another proarrhythmic effect.
- This last effect (ie, facilitating conversion of AFib to AFlutter) — may prove especially problematic if Flecainide is given without associated use of a rate-slowing agent, such as a ß-blocker (ie, slowing of the atrial rate of AFlutter may facilitate 1:1 AV conduction of a wide tachycardia that looks like VT).
- NOTE: Because of Flecainide’s adverse effect on conduction through atrial, ventricular and His-Purkinje tissue — the usual diagnostic and therapeutic effects of antiarrhythmic agents may be much less effective (if they are effective at all). This probably accounts for the refractoriness of Flecainide-induced proarrhythmia to antiarrhythmic treatment.
=====================================
Today's CASE Continues:
The tracing shown in Figure-8 was obtained several minutes after spontaneous conversion of the WCT rhythm that we showed in Figure-4.
- How would you interpret the rhythm in ECG #5?
-USE.png) |
| Figure-8: This tracing was obtained shortly after spontaneous conversion of the WCT rhythm seen earlier. |
- Note that the QRS remains markedly widened, as it was during the WCT.
- Unlike sinus rhythm — upright deflections that look like P waves appear before each QRS complex not only in lead II — but also in all chest leads except V6 — with these deflections being larger in the chest leads than in lead II.
- In addition — the ventricular rate in Figure-8 would be relatively fast for a post-conversion sinus rhythm.
- The reason interpretation of ECG #5 is so challenging — is that the distance between flutter waves and neighboring QRS complexes has changed compared to prior telemetry tracings. This shifting relationship between flutter waves and neighboring QRS complexes is common — and simply results from slight changes in the atrial flutter rate.
- To emphasize: Clinical context is KEY for suspecting this rhythm is 2:1 AFlutter! Since all other telemetry recordings are the result of differing AFlutter conduction ratios — the chances are great that the rhythm in ECG #5 will also represent AFlutter. As a result — We looked especially carefully for subtle signs of AFlutter (ie, the relatively fast ventricular rate that would be unusual for a post-conversion sinus rhythm — and — the larger size of atrial deflections in most chest leads compared to lead II ).
- Using calipers facilitates "walking out" regular 2:1 atrial activity that is best seen in lead V1 (RED arrows in this lead highlighting perfectly spaced indication of ongoing 2:1 atrial activity — with extra peaking in each T wave resulting from hidden flutter waves).
-USE.png) |
| Figure-9: RED arrows highlight 2:1 AFlutter (with peaking of each T wave in lead V1 resulting from hidden flutter waves). |
- The underlying rhythm throughout today's case was AFlutter — often with 2:1 AV conduction (and a regular R-R interval) — but alternating with variable ratios of multilevel Wenckebach conduction out of the AV node.
- This patient had been on longterm Flecainide — but was not receiving a ß-blocker! This facilitated AFlutter episodes with 1:1 AV conduction.
- Marked QRS widening with an unusual QRS morphology (that resembled VT) — was the result of Flecainide toxicity.
- Flecainide was discontinued. A ß-blocker was started. After withdrawing Flecainide — the atrial flutter rate increased, approaching a rate of 300/minute.
- Despite ß-blocker treatment — 2:1 AV conduction persisted, with a ventricular response of ~150/minute. The decision was then made to electrically cardiovert the patient, who was then referred for AFlutter ablation.
- Diagnosis of the various presentations of AFlutter may be challenging — especially when flutter waves are not readily visible in the usual leads. The best way to avoid overlooking AFlutter — is to think of this diagnosis whenever the clinical picture does not "fit" with the ECG rhythm.
- Flutter waves may simulate the sinus P waves of sinus tachycardia (especially when every other flutter wave is hidden within the preceding QRS or ST-T wave).
- Be aware of the signs of Flecainide toxicity — especially of the tendency to precipitate 1:1 AV conduction of AFlutter in a patient on Flecainide without associated use of a rate-slowing agent (such as a ß-blocker).
- Regardless of how bizarre QRS morphology during a WCT rhythm may be — Consider 1:1 AV conduction of AFlutter (and not VT) if the patient has been on Flecainide for control of chronic AFib (especially if not also on a rate-slowing agent).
- Grauer: Because my "ECG brain" has been wired for interpretation of ECGs at the 25 mm/second speed (that is standard in the U.S. and in most of the world) — My routine is to selectively reduce the width of such tracings by 50% to compensate for the 50 mm/second speed routinely used with the Cabrera format. This has been done in Figure-1.
- Outlined in BLUE just above lead V1 — are several ECG grid boxes to facilitate recognizing that the R-R interval in ECG #1 is approximately 3 large boxes in duration — corresponding to a rate of ~100/minute for the rhythm in Figure-1.
- Given globalization of our world — we favor familiarization with different recording formats (For detailed review of the Cabrera Format — Check out Dr. Grauer's Comment at the bottom of the page in the October 26, 2020 post in Dr. Smith's ECG Blog).
- Other than sinus rhythm — What else do you see in ECG #1?
|
| Figure-1: The initial ECG in today's case. |
- The rate of ~100/minute would be fast for an 80-something year old adult — unless something acute is going on (or unless there is really 2:1 AV conduction).
- There is no upright P wave in lead II (and other than some broad, low amplitude deflections before the QRS in some chest leads — really no clear indication of P waves in other leads). KEY Point: Unless there is lead reversal or dextrocardia — the P wave should always be upright in lead II if the rhythm is sinus.
- Sinus P waves are usually not all positive in lead V1 (unless there is RAA).
- The presence of a pseudo-r' deflection in lead V1 (as we see in Figure-2) — is a common "hiding place" for either extra or retrograde P waves.
- Grauer: My “Go To” Leads when looking for less obvious atrial activity in a supraventricular rhythm — are leads II and V1 (as the best leads to look at first) — but also leads III,aVF and aVR.
- That said — the rhythm in Figure-2 looks supraventricular (with a nonspecific conduction defect) — given 2:1 atrial activity in which the PR interval is constant before each QRS.
- There are nonspecific ST-T wave changes that do not appear to be acute.
- We have described a regular supraventricular rhythm with 2:1 AV conduction for the rhythm that appears in Figure-2.
- The ventricular rate is ~100/minute.
- Since there are 2 P waves within each R-R interval — the atrial rate must therefore be twice the ventricular rate, or ~200/minute.
- The differential diagnosis in Figure-2 is between i) ATach (Atrial Tachycardia) vs ii) AFlutter (Atrial Flutter). Although a subtle "sawtooth" pattern does appear to be present in the inferior leads — a ventricular response of ~200/minute would be slow for untreated AFlutter ...
|
| Figure-2: Colored arrows highlight flutter waves, with 2:1 AV conduction. |
- On questioning — the patient reports intermittent palpitations in recent months.
- His current hospital admission was for suspected SSS — BEGIN HERE!
The patient in today's case is a 80 something male with a medical history of hypertension and paroxysmal atrial fibrillation. He has been well controlled on flecainide therapy for many years. He presented to the emergency department due to syncope while at rest. Below in Figure-1 is the presentation ECG.
|
| Figure-3: Rhythm captured on telemetry. (Recording speed = 25 mm/second.) |
- XXXX
|
| Figure-4: Spontaneous conversion of the WCT rhythm shown in Figure-3. |
|
| Figure-5: An additional rhythm recorded on telemetry. |
XXXXXXXX
|
| Figure-6: I've labeled atrial activity in ECG #4. |
XXXXXXXXX
|
| Figure-7: Proposed laddergram for ECG #4 (See text). |
Let us go back to the WCT and have a closer look at the RR intervals before and after termination. Before termination, the R-R intervals of the WCT is about 360ms (9 small boxes). After the termination there is an almost perfect doubling of the R-R interval. This is consistent with 1:1 and then 2:1 conduction of atrial arrhythmia.
=======================================
MAGNUS — The R-R interval is different (slightly-but-diffferent) for each of the 5 complexes after the tachycardia. So it is not true to say, "there is almost perfect doubling of the R-R interval". Therefore, I omitted this Figure ... KEN (1/4/2025 @ 5pm EST).
=======================================

|
| Figure-8: This rhythm strip was obtained several minutes after spontaneous cardioversion of |
- Clinical picture did not fit sinus tachycardia
- An all-upright sinus P wave in lead V1 is not common (BUT IT CAN OCCUR!). In contrast — atrial morphology in lead V1 is perfectly consistent with atrial flutter.
- Terminal portion of V1 has much more than just "the look" of hidden atrial activity — if you take your calipers — there is an identically shaped notch right after the QRS in your magnified Figure-4. I was 99+% certain of 2:1 AFlutter as soon as I saw that — :)
- 2:1 flutter can sometimes be difficult to discern from sinus tachycardia. Always consider this arrhythmia if clinical picture does not fit with sinus tachycardia.MAGNUS — To me, we are really talking about the "Bix Rule" — in that the PR interval of a sinus rhythm typically shortens with tachycardia — yet the PR interval "looks long" in Figure-1 (I am unable to calculate the actual PR interval — but doing so would add to your discussion — since it is the "Bix Rule" that has tipped me off countless times that sinus tach is not present). IF interested — I review the BIX RULE in my ECG Blog #227 ( https://tinyurl.com/KG-Blog-227 )
- Consider atrial flutter or atrial tachycardia if the P waves are all-upright in V1.
- Flecainide may slow atrial flutter sufficiently to allow 1:1 AV conduction. Never prescribe flecainide without give av nodal blockers to patients with atrial fibrillation or atrial flutter.
- For clarity — I’ve put the 1st and 3rd ECGs in this case together (Figure-1) — and have labeled what for me constitute KEY findings.
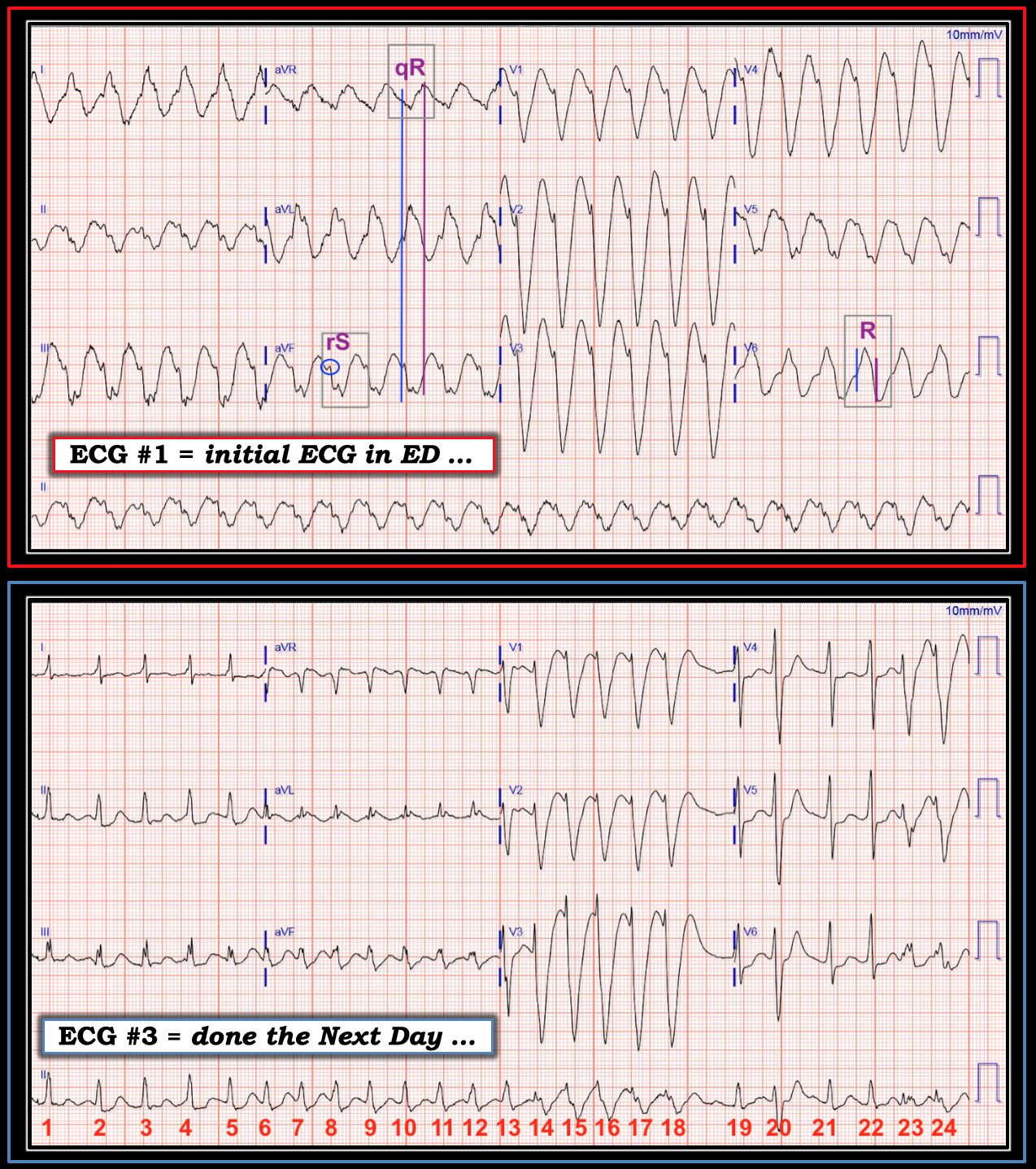 |
| Figure-1: TOP — ECG #1 ( = the initial ECG performed in the ED). BOTTOM — ECG #3 in this case (done the next day). Key findings are labeled. |
- BUT — this patient was known to be on Flecainide for treatment of PAF (Paroxysmal AFib). And, among potential manifestations of Flecainide Toxicity are: i) QRS widening which may be marked, often with bizarre QRS morphology; ii) Slowing of conduction in atrial and ventricular tissue, as well as in the His-Purkinje system; iii) VT, as a proarrhythmic effect; and, iv) facilitating conversion of AFib to AFlutter, as another proarrhythmic effect.
COMMENT: Awareness of these potential manifestations of Flecainide Toxicity should alter our use of traditional assessment factors for distinguishing between SVT vs VT. For example:
- Statistical likelihood that the regular WCT in ECG #1 might be AFlutter (instead of VT) is greatly increased in a patient with AFib who is taking Flecainide. In such a patient, we need to significantly adjust downward the statistical likelihood that a regular WCT without P waves is VT.
- If AFlutter does develop as Flecainide-induced proarrhythmia — we should expect unusual QRS morphology with marked QRS widening. As a result — use of traditional QRS morphology characteristics will usually not be helpful in distinguishing between VT vs SVT, because the QRS complex in Flecainide-induced AFlutter is unlikely to resemble any form of conduction defect (CLICK HERE — for my approach using QRS morphology with WCT).
- Because of Flecainide’s adverse effect on conduction through atrial, ventricular and His-Purkinje tissue — the usual diagnostic and therapeutic effects of antiarrhythmic agents may be much less effective (if they are effective at all). This probably accounts for the refractoriness of Flecainide-induced proarrhythmia to antiarrhythmic treatment. In this particular case — it may account for diagnostic failure of Adenosine to slow AV conduction in a patient with AFlutter.
- Perhaps flutter waves are hidden within artifact, within ST-T waves, and by the wide, bizarre QRS complexes?
- Perhaps the reason the rhythm in ECG #1 is regular, but without 2:1 flutter waves — is that we are seeing 1:1 AFlutter, due to marked atrial slowing from Flecainide toxicity?
- Measurements regarding slow initial depolarization, and delay until peak negativity are irrelevant for distinguishing SVT from VT in light of Flecainide toxicity. That’s because both VT and Flecainide-induced AFlutter demonstrate delay in ventricular conduction.
- The initial deflection in lead aVR is not positive, but negative (See vertical BLUE line showing that initial negativity in aVR corresponds with onset of the QRS complex in simultaneously-obtained leads aVL and aVF). This is far less predictive of VT than if the QRS complex in aVR was completely positive.
- Extreme axis deviation in the frontal plane is not present — because a small-but-definitely-present initial r wave is seen in all 3 inferior leads (See within the BLUE circle in lead aVF). Specificity of frontal plane axis deviation is unacceptably poor as a sign for distinguishing SVT from VT when the QRS complex is not all negative in either lead I or in lead aVF.
- QRS morphology in the chest leads is consistent with a supraventricular etiology — since a monophasic R wave is present in lead V6.
- Finally — I believe a plausible pattern for progressive QRS widening with a rate-related component of aberrant conduction is seen in this patient with Flecainide-induced proarrhythmia.
- Note QRS widening for beats #14-thru-18 in ECG #3. This illustrates the use-dependent phenomenon mentioned earlier by Dr. Walsh (greater effect on QRS widening from Flecainide toxicity at faster heart rates). That this 5-beat run is still AFib is suggested by slight-but-real irregularity to caliper measurement of the R-R interval during these 5 beats (the rhythm in ECG #1 was virtually clockwork regular!).
- Note that beat #19 in ECG #3 narrows! This supports a rate-related aberrancy component — because of the brief pause just prior to beat #19.
- The QRS widens a bit in beat #20 — compared to the narrower QRS of neighboring beats #19, 21 and 22. This is again consistent with a rate-related aberrancy component by the Ashman phenomenon (in which aberrancy follows a relative pause).
- Measuring with calipers, the rate then speeds up slightly for beats #23 and 24 — and we once again see QRS widening (ie, rate-related aberrancy) for beats #23 and 24.
- Now look at the long lead II at the bottom of ECG #3 in its entirety. Note how the rate of the underlying AFib begins SLOWER than 150/minute for the first few beats! Thus, the rate for these first few beats is slower than the 150/minute rate seen in ECG #1. That’s why the QRS complex is much narrower (virtually of normal duration) for beats #1-6 in ECG #3.
- As the rate of AFib gradually (and progressively) increases — the QRS progressively widens, until it becomes very wide for beats #14-thru-18.
- For as wide as the QRS is for beats #14-thru-18 (I measure 0.22 second) — the QRS was wider still in ECG #1 (I measure 0.25 second), in which the tachycardia is sustained.
- The QRS was also wide in ECG #2 (I measure 0.12 second) — which was the tracing recorded right after synchronized cardioversion resulted in sinus rhythm. Presumably, the reason the QRS is “only” 0.12 second in ECG #2 (instead of the 0.25 second for the QRS in ECG #1) — is that the rate in sinus rhythm is now much slower.
- Both QRS duration and QRS morphology in the long lead II of ECG #2 — is very similar to QRS duration and QRS morphology in the long lead II of ECG #3 for beats # 5, 6; and 19, 21, 22.
- ALL points in the above bullets are consistent with what I’d expect in a patient with QRS widening from Flecainide toxicity + a rate-related component of aberrant conduction. Rate-related relationships are not perfect (they never are with rate-related aberrancy — CLICK HERE) — but the overall “theme” of what we see in this case ( = in My Opinion) is certainly consistent with this phenomenon.
- Finally — If one “steps back” to attempt an overall perspective of QRS morphology in multiple leads on these 3 tracings as heart rate increases and the QRS widens (ie, sequentially looking at the less wide QRS in sinus rhythm with ECG #2 — then the changing rates of the AFib tracing in ECG #3 — and then the widest QRS in ECG #1) — I see elements of similarity in QRS morphology in many leads, as I might expect from toxicity-induced QRS widening with rate-related changes. I just would not expect the above findings if ECG #1 was VT …
===================================
MY Comment, by KEN GRAUER, MD (5/21/2023):
https://hqmeded-ecg.blogspot.com/2023/05/an-elderly-patient-with-syncpe-dyspnea.html
My comment reviews Flecainide Toxicity - MUST USE!
===================================
- As per Dr. Smith — Although ECG #1 manifests eye-catching ST elevation in anterior leads V1-thru-V4 — this tracing is much more likely to represent Flecainide Toxicity, and not an acute OMI.
- That said, even more concerning to me than the anterior lead findings — is the shape of the ST elevation in lead aVL — and the ledge-like reciprocal ST depression in leads III, aVF and V6.
- To Emphasize: I completely agree with Dr. Smith that the ECG abnormalities in Figure-1 will most probably resolve as this patient's Flecainide toxicity is treated — but ruling out the possibility of superimposed infarction with serial troponins will be prudent.
- Depressed contractility; hypotension (negative inotropic effect).
- Depression of all major conduction pathways (ie, in the AV Node; His-Purkinje system, in the ventricles). This may result in a series of conduction disorders including various forms of AV block; bundle branch blocks; impaired pacemaker function. The QRS may be markedly widened and bizarre in morphology.
- Flecainide Toxicity is suggested when: i) There is ≥50% increase in QRS duration (typically producing a QRS ≥0.18 second); and/or, ii) A ≥30% increase in PR interval duration (typically to a PR ≥0.26 second). The QTc may also be increased (though much of this effect is the result of QRS rather than QT prolongation).
- Lethal arrhythmias may be a terminal event (VT/VFib; Asystole).
- BOTTOM Line: As per Dr. Smith — Flecainide toxicity is the most likely primary cause of the ECG findings in Figure-1.
-USE.png) |
| Figure-1: The initial ECG in today's case. |
===================================
MY Comment, by KEN GRAUER, MD (11/24/2020):
===================================
MY Comment, by KEN GRAUER, MD (6/3/2024):
- For clarity in Figure-1 — I have labeled the initial ECG, and added a laddergram to illustrate the mechanism of the rhythm
 |
| Figure-1: I’ve labeled the initial ECG in Cast #2 — and have added a laddergram. (To improve visualization — I've digitized the original ECG using PMcardio). |
- The reason diagnosis of acute LAD OMI is challenging in Case #2 — is superposition of flutter waves on top of the underlying ST-T wave. That said — RED arrows in leads V1 and V2 in Figure-1 clearly show ST segment coving and elevation (that should not be there with RBBB — which normally shows ST depression in these leads). Careful scrutiny of the ECG baseline in these leads (within the RED rectangle) reveals a clear difference compared to the baseline away from the ST segments.
- More subtle, but still definitely present — is the ST elevation also in lead aVL (RED arrows in this lead) — with this subtle ST elevation in aVL most noticeable when compared to the ECG baseline away from the QRS in lead aVL.
- BLUE arrows in lead III and lead aVF — reveal subtle-but-definitely present reciprocal ST depression (again, best appreciated when the "dip" in the ST segments highlighted by the BLUE arrows in these leads is compared to the ECG baseline away from QRS complexes).
- BOTTOM Line: The combination of abnormal ST coving and elevation in leads V1,V2 and aVL — in association with reciprocal ST depression in inferior leads III and aVF — in this patient with new chest pain — is absolutely diagnostic of proximal LAD OMI.
- Although not all R-R intervals in Figure-1 are equal — there are only 2 different R-R interval durations — and these 2 R-R interval durations repeat! The shorter R-R interval separates beats #2-3; 4-5; and 7-8. The longer R-R interval separates beats #1-2; 3-4; 5-6; 6-7; 8-9; 9-10; 10-11; 11-12; and 12-13.
- KEY Point: As I've illustrated in a number of previous Blog posts — AFlutter commonly manifests Wenckebach conduction. Technically — this is not a conduction "block", but rather expected reduced conduction by an AV node presented with extremely rapid flutter impulses that are too fast to conduct them all! (~300/minute in today's case!).
- More than just 2 families of similar R-R intervals — the PR interval in front of each of the QRS complexes in the larger R-R interval group is the same! (ie, the PR interval that begins with each of the BLUE lines).
- Similarly — the PR interval in front of each of the QRS complexes in the shorter R-R interval group is also the same! (ie, the PR interval that begins with each of the PURPLE lines).
- PEARL: It took me less than 5 seconds to recognize this repetitive relationship between these 2 families of R-R intervals — and the finding of 2 similar PR intervals preceding both shorter and longer R-R intervals. This is not by chance — and with AFlutter, is virtually diagnostic of dual-level AV Wenckebach conduction in a patient with AFlutter! (See My Comment and laddergram in the November 24, 2020 post and the May 26, 2023 post, regarding the concept of dual AV nodal Wenckebach conduction).
- I've drawn a laddergram in Figure-1 to illustrate my proposed mechanism for this rhythm. Keep in mind that because of "concealed" conduction (ie, atrial impulses bombarding the AV node) — it is usually not the flutter wave closest to a QRS that conducts. Thus, there is dual-level Wencekbach conduction out of the AV node — with 2:1 conduction in the upper AV nodal level — and 3:2 alternating with 2:1 conduction in the lower AV nodal level.
- To EMPHASIZE — There is no need to dwell on the sophisticated mechanism of the rhythm in this 2nd Case. What I do want to emphasize — is to appreciate that AFlutter (as well as ATach) will commonly manifest Wenckebach conduction at 1 or more levels out of the AV node — and that simply by appreciating that a pattern does exist to the rhythm (as I illustrate above) — you can within seconds identify Wenckebach conduction as an expected consequence of these rhythms.
- Finally, to emphasize — This Wenckebach conduction out of the AV node is not an AV "block" per se — and chances are excellent that normal AV conduction will resume once sinus rhythm is restored!
-USE.png) |
| Figure-1: The initial ECG in today's case. (To improve visualization — I've digitized the original ECG using PMcardio). |
Written by Magnus Nossen (LATEST DRAFT !!! )==================
Written by Magnus Nossen
- You KNOW I am totally supportive of Cabrera format — and especially of familiarizing Blog readers with this (and other) formats. That said — I'll guess that 90+% of Blog readers do not encounter Cabrera format often. Most also are probably much more familiar with 25 mm/sec speed. Therefore — my suggestion is that you always reread your text with that type of reader in mind ... (I fully acknowledge that on the presentation ECG below — I have NO idea of what is going on because I think ( ??? ) that it is recorded at 50 mm/sec. speed — and my "brain" just doesn't "work" until I reduce width by 50%. And, since this is the KEY 1st tracing in your Blog post, my suggestion is that it is FINE to show this tracing first as is (specifying that the speed is 50 mm/sec).
- BUT — I would then ALSO post this same 1st ECG at 25 mm/sec.
- I think it is especially important to clearly indicate recording speed ON each ECG (especially since you have some 25 mm/sec tracings and some at 50 mm/sec).
- In my opinion — ALL Figures should always be labeled ON the actual ECG. My reasons for saying this are: i) It is otherwise confusing to me in places of your text which tracing you are talking about; and ii) When readers click on Figures to magnify them — especially in your cases where there are multiple Figures — it gets very confusing as to which Figure is which (because when clicked on to magnify — your legend does not show).
- MAGNUS — Below is the way I would write this up. Others do it differently — so I am merely offering my suggestions. It is UP TO YOU as to how you decide to do this.
- P.S. — Let me know if you need help with the Figures. If so — I'd need to have your best copy both in labeled (to orient me) and unlabeled form.
The patient in today's case is a 80 something male with a medical history of hypertension and paroxysmal atrial fibrillation. He has been well controlled on flecainide therapy for many years. He presented to the emergency department due to syncope while at rest. Below in Figure-1 is the presentation ECG.
What do you think?
 |
| ECG #1 |
{kind=link}
 |
| Figure-1: The initial ECG in today's case (recorded at 50 mm/sec). |
 |
| Figure-1a: The initial ECG in today's case (corrected to a recording speed of 25 mm/sec). |
The above ECG shows a regular rhythm with a QRS duration of about 120msec. The heart rate is approximately 100 beats per minute. There is a normal axis at 0 degrees. (Actually the frontal plane axis is about 0 degrees — given all pos in lead I but isoelectric in lead aVF. So of course a 0 degrees axis is "normal" — but it IS remarkable in being "different" than the usual axis. Problem could be easily solved by saying it's a normal axis at 0 degrees). There is no evidence of ischemia. (I'd start a new paragraph here) On questioning, the patient reported intermittent palpitations for the last few months. He was admitted to the hospital with a suspected diagnosis of sick sinus syndrome. ("With tachycardia" is not a new sentence — but rather a continuation from "sick sinus syndrome" ). With tachycardic spells (accounting for palpitations) and bradycardic spells likely being the cause of the recent syncope.
While on TM the following arrhythmia was captured: (Figure-2)
 |
| ECG #2 |
{kind=link}

- I really think it important to acknowledge to your reader these challenges. If it were me — I probably would opt for a more readable tracing (ie, using 5 leads from aVL-to-aVF) — but it is FINE to show all 12 leads as you do IF you "comfort" the reader as to the problematic aspects. I'd do this by simply stating something like, "Unfortunately — there is overlap of the 5 chest leads that we see — and we have lost most of the lead V6 recording. That said — interpretation of this arrhythmia should still be possible".
This ECG shows a wide complex tachycardia with a heart rate of around 180 beats per minute. During the WCT the patient had a near syncopal episode. There was spontaneous termination? termination of WCT within approximately three minutes. The termination is shown below in Figure-3.
 |
| ECG #3 |
{kind=link}

Discussion: I saw ECG number 1 by itself with the information that the patient was an elderly male on flecainide treatment presenting due to syncope. Instead, I'd phrase it more like this, "I initially saw the ECG in Figure-1, knowing only that the patient was an elderly man on flecainide, who presented to ED for syncope. I was told he had an episode of ventricular tachycardia. I was not convinced the WCT was ventricular in origin. Why did I think this? (this is the perfect place to use italics = Why did I think this? .
I'd leave a little space before you give the answer. To prevent a "spoiler" — just skip a few lines and add a heading in bold ...
MY Thoughts on the ECG in Figure-2:
Lead V1 in the initial ECG in todays case made me doubt the diagnosis of VT. Let us have a closer look at V1 from the presentation ECG. Below I have magnified leads V1-V2. Let's look closer at a magnifed view of leads V1 and V2 from today's initial tracing (Figure-4). The This ECG was interpreted as showing sinus tachycardia.
Remember! It would be very unlikely for an 80-something to have a resting sinus rate of 100bpm in the presence of negative chronotropic medication unless there is some underlying cause like infection, anemia, hypoxemia or other illness that leads to an increase in sympathetic tone.
What at first glance could be mistaken for sinus tachycardia is in fact not. There are deflections at the end of the QRS (best seen in V1). Below I have marked atrial activity with arrows.

 |
| Figure-4: Magnified view of leads V1,V2 from Figure-1. (Recording speed was 50 mm/sec.). |
In order to prove beyond any doubt that this is not sinus tachycardia but rather 2:1 atrial flutter, I went to the telemetry station and found the ECG below in Figure-5. ECG. This ECG shows a regular atrial arrhythmia with a cycle length in the atria of about 320msec. There is varying degree of AV block BEST not to refer to variable conduction with AFlutter as a form of "block" — because "block" implies pathology, and variable conduction with AFlutter is physiologic (and usually goes away if you convert the rhythm to sinus) with predominant 2:1 and sometimes 3:1 conduction. (So this is actually intermittent dual-level AV block with Wenckebach conduction out of the AV node. I can eventually draw a laddergram of this interesting rhythm. You could simplify your description by simply saying "there is AFlutter with predominant 2:1 AV conduction, with some variable conduction out of the AV node" ).


Magnus — since you have mixed recording speeds on today's tracings — for clarity I think it important ON the actually ECG to indicate the recording speed used for each tracing. This tracing did have it — but the writing was tiny and blurred. EASIEST approach — is WHITE OUT that writing — don't worry about the 10mm/mV — but write clearly, "25 mm/sec." — :)

Let us go back to the WCT and have a closer look at the RR intervals before and after termination. Before termination, the R-R intervals of the WCT is about 360ms. As you can see there is a doubling of the R-R intervals from about 360msec to 720msec. This is consistent with 1:1 and then 2:1 conduction of atrial arrhythmia.
When the cycle length in atria prolongs this may lead to 1:1 conduction. The patient in today's case was not prescribed an AV nodal blocker, which is mandatory when treating atrial fibrillation and atrial flutter with flecainide. Patients need AV nodal blockers precisely to prevent what happened to this patient.
MAGNUS — I feel the above 2 paragraphs and construction of the figure shown here needs revision. The problems are that after beat #12 — the R-R interval is NOT regular (there is slight R-R interval variation, not only for the R-R interval between #12-13, but beyond that). Also — I am not convinced that after beat #12 that there is AFlutter ... (it could be AFib). Lead V5 is just not convincing to me of flutter waves (even going back to Fig. 1 when we have 2:1 clearly seen in lead V1 — I did NOT see convincing 2:1 atrial activity in lead V5 ...
 |

Conclusion: This is YOUR theory — but are you 1,000% certain? EASILY fixd by beginning by say, "I suspect that The wide complex tachycardia (WCT) was due to intermittent 1:1 conducted 1:1 AV conduction of atrial flutter. (MAGNUS — I'm a bit confused between what we think is rate-related aberrant conduction vs QRS widening produced by flecainide ...) atrial arrhythmia with aberrant conduction. Flecainide was discontinued and a betablocker was started. After the flecainide treatment was withdrawn the atrial cycle length I'm confused about what cycle length you are talking about? Is this the P-P interval? Might be much easier to conceptualize if you talk about the approximate change in atrial rate of the underlying AFlutter (ie, the atrial flutter rate went from ~300/minute to XXX/minute — whatever those rates which I have not calculated happened to be). shortened significantly and the patient despite betablocker treatment remained in a 2:1 conducted atrial flutter AFlutter with 2:1 AV conduct, with a ventricular response of at about 140 beats per minute. He was later cardioverted and referred for atrial flutter ablation.
Looks like you are summarizing ... — so I'd skip a few lines and add a brief heading ...
In Summary: The initial ECG in todays case was initially interpreted as showing sinus tachycardia. What made me this this was unlikely? There are three main reasons.
- Clinical picture did not fit sinus tachycardia
- All-upright P-waves in V1 does not occur in sinus rhythm An all-upright sinus P wave in lead V1 is not common (BUT IT CAN OCCUR!). In contrast — atrial morphology in lead V1 is perfectly consistent with AFlutter.(but does occur with flutter!)
- Terminal portion of V1 had the look of «hidden» atrial activity. Much more than just "the look" of hidden atrial activity — IF you take your calipers — there is an IDENTALLY shaped notch right after the QRS in your magnified Figure-4. I was 99+% certain of 2:1 AFlutter as soon as I saw that — :)
- 2:1 flutter can sometimes be difficult to discern from sinus tachycardia. Always consider this arrhythmia if clinical picture does not fit with sinus tachycardia. MAGNUS — To me, we are really talking about the "Bix Rule" — in that the PR interval of a sinus rhythm typically shortens with tachycardia — yet the PR interval "looks long" in Figure-1 (I am unable to calculate the actual PR interval — but doing so would add to your discussion — since it is the "Bix Rule" that has tipped me off countless times that sinus tach is not present). IF interested — I review the BIX RULE in my ECG Blog #227 ( https://tinyurl.com/KG-Blog-227 )
Always considerConsider atrial flutter or atrial tachycardia if P wave is all-upright in V1.- Flecainide may slow atrial flutter sufficiently to allow 1:1 AV conduction. Never prescribe flecainide without give av nodal blockers to patients with atrial fibrillation or atrial flutter.
Written by Magnus Nossen
The patient in today's case is a 80 something male with a medical history of hypertension and paroxysmal atrial fibrillation. He has been well controlled on flecainide therapy for many years. He presented to the emergency department due to syncope while at rest. Below is the presentation ECG.
What do you think?
|
| ECG #1 |
The above ECG shows a regular rhythm with a QRS duration of about 120msec. The heart rate is approximately 100 beats per minute. There is a normal axis. There is no evidence of ischemia. On questioning, the patient reported intermittent palpitations for the last few months. He was admitted to the hospital with a suspected diagnosis of sick sinus syndrome. With tachycardic spells (accounting for palpitations) and bradycardic spells likely being the cause of the recent syncope.
While on TM the following arrhythmia was captured:
|
| ECG #2 |
This ECG shows a wide complex tachycardia with a heart rate of around 180 beats per minute. During the WCT the patient had a near syncopal episode. There was termination of WCT within approximately three minutes. The termination is shown below.
|
| ECG #3 |
Discussion: I saw ECG number 1 by itself with the information that the patient was an elderly male on flecainide treatment presenting due to syncope. I was told he had an episode of ventricular tachycardia. I was not convinced the WCT was ventricular in origin. Why did I think this?
Lead V1 in the initial ECG in todays case made me doubt the diagnosis of VT, Let us have a closer look at V1 from the presentation ECG. Below I have magnified leads V1-V2. The ECG was interpreted as showing sinus tachycardia.
Remember! It would be very unlikely for an 80-something to have a resting sinus rate of 100bpm in the presence of negative chronotropic medication unless there is some underlying cause like infection, anemia, hypoxemia or other illness that leads to an increase in sympathetic tone.
What at first glance could be mistaken for sinus tachycardia is in fact not. There are deflections at the end of the QRS (best seen in V1). Below I have marked atrial activity with arrows.
In order to prove beyond any doubt that this is not sinus tachycardia but rather 2:1 atrial flutter, I went to the telemetry station and found the below ECG. This ECG shows a regular atrial arrhythmia with a cycle length in the atria of about 320msec. There is varying degree of AV block with predominant 2:1 and sometimes 3:1 conduction.
Let us go back to the WCT and have a closer look at the RR intervals before and after termination. Before termination, the R-R intervals of the WCT is about 360ms. As you can see there is a doubling of the R-R intervals from about 360msec to 720msec. This is consistent with 1:1 and then 2:1 conduction of atrial arrhythmia.
When the cycle length in atria prolongs this may lead to 1:1 conduction. The patient in today's case was not prescribed an AV nodal blocker, which is mandatory when treating atrial fibrillation and atrial flutter with flecainide. Patients need AV nodal blockers precisely to prevent what happened to this patient.
|
Conclusion: The wide complex tachycardia (WCT) was due to intermittent 1:1 conducted atrial arrhythmia with aberrant conduction. Flecainide was discontinued and betablocker was started. After the flecainide treatment was withdrawn the atrial cycle length shortened significantly and the patient despite betablocker treatment remained in a 2:1 conducted atrial flutter at about 140 beats per minute. He was later cardioverted and referred for atrial flutter ablation.
The initial ECG in todays case was initially interpreted as showing sinus tachycardia. What made me this this was unlikely? There are three main reasons.
- Clinical picture did not fit sinus tachycardia
- All-upright P-waves in V1 does not occur in sinus rhythm(but does occur with flutter!)
- Terminal portion of V1 had the look of «hidden» atrial activity.
- 2:1 flutter can sometimes be difficult to discern from sinus tachycardia. Always consider this arrhythmia if clinical picture does not fit with sinus tachycardia.
- Always consider flutter or atrial tachycardia if P wave is all-upright in V1.
- Flecainide may slow atrial flutter sufficiently to allow 1:1 AV conduction. Never prescribe flecainide without give av nodal blockers to patients with atrial fibrillation or atrial flutter.
No comments:
Post a Comment