===================================
Comment by KEN GRAUER, MD (6/22/2022):
===================================
An important part of the process of assessing serial ECGs — is comparison with a prior ("baseline" ) tracing. The goal of determining which changes are new was instantly evident in today's case by review of the old ECG ( = the 2nd ECG shown above in Dr. Smith's discussion of this patient's serial tracings).
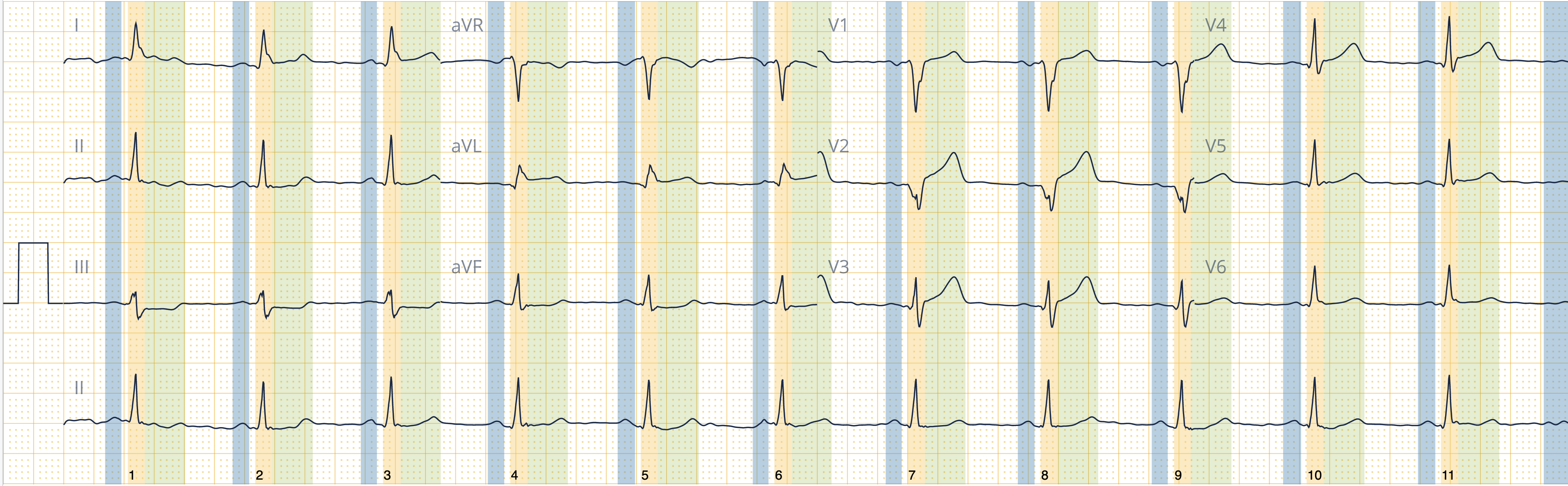
I found the Old ECG in today's case to be fascinating — so I focus my comment on its analysis. For clarity — I've reproduced this 2nd tracing in Figure-1. At the time this Old ECG was done — the patient had a pacemaker. As per Dr. Smith — the rhythm in ECG #2 shows intermittent ventricular pacing with evidence of infero-postero infarction at some point in time.
QUESTIONS:
No clinical information was available in association with the ECG in Figure-1. All we know — is that this ECG was recorded at some point in the past.
- How would you “date” the infarction in Figure-1?
- Is the pacemaker functioning appropriately?
- What is the underlying cardiac rhythm? (ie, WHY do you think the pacemaker was needed?).
-USE.png) |
| Figure-1: The previous ECG in today's case. (To improve visualization — I've digitized the original ECG using PMcardio). |
MY Thoughts on the Old ECG:
The art and science of cardiac pacing continues with breathtaking advances. It is no longer easy (or even possible) to fully assess pacemaker function solely from the ECG without knowledge of pacing specifications for that particular patient. That said — we often can get a quick idea as to how a pacemaker is functioning, especially when one or more spontaneous beats are present. For the ECG that appears in Figure-1 — there is more to be learned!
- The "good news" — is that modern pacemakers can be interrogated remotely by means of a wireless, telemetered, external programming device (Brief review by Safavi-Naeini and Saeed — Texas Heart Inst J 43:415-418, 2016 on the basics of pacemaker troubleshooting).
- The 2nd piece of "good news" — is that modern pacemakers are truly amazing devices with an astonishing performance record. Pacemaker malfunction does occur (and it is important to recognize this when it happens) — but most of the time, the pacemaker will be right! So I generally begin my assessment of pacemaker tracings with the mindset that even when I see unusual or unexpected findings — there may be a physiologic reason for why the pacemaker is appropriately functioning in this way (the details of which can then be sorted out when the pacemaker is interrogated).
Assessing the Pacemaker:
In Figure-2 — I've labeled the long lead II rhythm strip from ECG #2.
- RED arrows in Figure-2 reveal that there is an underlying regular sinus rhythm in ECG #2. Note that the PR interval that precedes each of the narrow beats (ie, beats #1, 4, 7) is the same! Therefore — beats #1, 4 and 7 are sinus-conducted (albeit with a prolonged PR interval of 0.24 second = 1st-degree AV block).
- The vertical PINK lines in Figure-2 highlight pacemaker spikes. The fact that wide, paced complexes immediately follow pacemaker spikes to produce beats #2,3; 5,6; and 8 — confirms that there is at least some ventricular capture!
- The R-R interval of the first 3 pacemaker spikes is 6 large boxes. This corresponds to a pacing rate of 50/minute — which presumably is the rate the pacer was set at to fire if no spontaneous beats are sensed.
WHY does the 4th pacer spike occur early?
- Note that beat #4 is a spontaneous sinus-conducted beat! If the pacemaker was only sensing the QRS — then we would not see this 4th pacemaker spike that occurs just after beat #4!
- As stated a moment ago — spontaneous beats in Figure-2 are conducting with a prolonged PR interval. So it must be that the reason the 4th pacer spike in Figure-2 occurs early — is that there is dual chamber pacing (of both atria and ventricles) — and since no QRS complex was sensed after 0.23 second at this point in the cardiac cycle, the pacemaker fired. The 7th pacer spike in Figure-2 also occurs early for the same reason. This implies that the pacemaker is appropriately sensing the atria. (Simple adjustment could reprogram the pacer to accept a slightly longer PR interval before firing).
- That the pacer is appropriately sensing the ventricles — is evident from the 5th pacer spike — which once again waits the programmed amount of 6 large boxes after the previous pacer spike before firing. This provides the patient with a guaranteed ventricular rate of at least 50/minute — while still providing adequate opportunity for spontaneous conduction to occur.
-USE%20copy.png) |
| Figure-2: I've labeled P waves (RED arrows) and the pacemaker spikes (PINK lines) that are seen in the long lead II rhythm strip from ECG #2. |
How to "Date" the Infarction in Figure-1?
Now that we've determined from Figure-2 that beats #1, 4 and 7 are spontaneously conducted — We can return to Figure-1 to assess QRS morphology of these sinus-conducted beats.
- Focusing on beat #1 in leads II and III — reveals a large Q wave in lead III. The ST-T wave of these beats (as well as the ST-T for sinus-conducted beat #4 in lead aVF) looks hyperacute, albeit without frank ST elevation.
- Sinus-conducted beat #4 in lead aVL manifests reciprocal change (ie, mirror-image opposite ST-T wave depression — compared to the ST-T wave appearance in lead III). This suggests a recent inferior OMI (perhaps just after the stage of ST elevation). The hint of terminal T wave positivity in aVL (and of beginning T wave inversion in the inferior leads) may portend reperfusion.
- No spontaneous beats are seen corresponding to the 2 QRS complexes in leads V1,V2,V3 — but ST-T wave morphology of paced beats #5 and 6 suggests abnormal ST segment flattening with excessive T wave peaking (that is also seen for beat #8 in lead V4). I interpreted this ST-T wave appearance as indicative of posterior OMI reperfusion T waves.
- BOTTOM Line: My hunch is that there was a recent infero-postero OMI — and that we are now see reperfusion changes.
What is the Underlying Rhythm in Figure-1?
So WHY was the pacemaker needed for ECG-2? The answer to this is best explained by laddergram (Figure-3):
So WHY was the pacemaker needed for ECG-2? The answer to this is best explained by laddergram (Figure-3):
- For clarity — I labeled the sinus-conducted P waves in Figure-3 with RED arrows.
- YELLOW arrows highlight those P waves that are not conducted. Since some P waves are conducted but others aren't — some form of 2nd-degree AV block is present.
- PEARL: Since we know this patient has just had an infero-postero OMI — and there is group beating with sinus-conducted beats that manifest a narrow QRS with 1st-degree AV block — the odds are overwhelming that the type of conduction disturbance will turn out to be 2nd-degree AV block of the Mobitz I Type ( = AV Wenckebach)!
- GREEN arrows highlight non-conducted P waves that do not have a "chance" to conduct — because they either occur just before or just after paced beats.
- The small BLUE circles at the bottom of the laddergram correspond to pacer spikes. As already noted — the pacer spikes that appear just after sinus-conducted beats #1, 4 and 7 are appropriately sensing the preceding P wave — but do not pace the ventricles because of sinus conduction.
- BOTTOM Line: It is impossible to tell IF the GREEN arrow P waves would be able to conduct if given a chance to do so (which is why I added ??? in the AV nodal Tier of the laddergram). That said — as per the above Pearl — statistical odds overwhelmingly favor Mobitz I 2nd-degree AV block as the conduction disturbance — with the "good news" that AV Wenckebach in this setting often resolves as the patient's condition stabilizes.
.png) |
| Figure-3: My proposed laddergram for the rhythm in ECG #2 from Figure-1 |

XXXXXX
SSmith DRAFT (as of 6-21.21-2022):
The origin of these ECGs cannot be revealed. But I came across them while reading ECGs on the Cardiologs platform (Cardiologs uses Deep Learning to Interpret ECGs, and I am helping to train the Network)
Time 0:

Old ECG:

3 hours:

12 hours:
21 hours

No comments:
Post a Comment